INTRODUCTION
Toes play a significant role in stabilizing motor performance, including standing and walking.1) Toe muscle strength is a function of the toes. Older adults with decreased toe muscle strength have a higher risk of falling.2,3) Additionally, toe muscle strength in community-dwelling older adults has been associated with gait parameters, including decreased walking speed, swing time during walking, and shortened stride length.4) Furthermore, enhancing toe muscle strength improves balance ability.5) Therefore, toe muscle strength is associated with several physical functions.
While toe muscle strength has been assessed based on toe grip strength in the sitting position,1-5) walking, standing, and falling occur in the standing position. Moreover, toe muscle strength is enhanced by weight bearing in the upright position.6) Furthermore, we believe that assessment in the standing position is not only closer to the actual movement but also more reflective of an individual’s ability. Toe grip strength is typically evaluated by measuring the force of deep flexion of the toes. However, no toe-bending movements are observed during gait and balance. Previous studies have shown that the toes press against the floor surface during exercise.7) Furthermore, patients may complain of pain during toe grip strength assessment. Among interventions to increase toe grip strength, towel gathers are reportedly not only ineffective but also increase pain.8) To address these concerns, we devised a method to assess the toe pressure strength in the standing position. We previously reported the high reliability of measured toe pressure strength in the standing position and its criterion-related validity as a measure of muscle strength.9) In a study on older adults requiring long-term care, toe pressure strength in the standing position effectively discriminated the risk of falling.10) Therefore, measuring toe pressure strength in the standing position is an evaluation method that can be used in clinical practice.
Walking speed is a vital sign of physical function and an indicator of health status.11,12) It may decrease with age in the presence of motor or cardiovascular disorders.13,14) Maintaining walking speed is essential for older adults to perform activities of daily living without difficulty. For example, a certain walking speed is required to complete a pedestrian crossing in time. In addition, some situations require increased walking speed, including when others are waiting or when the time is short. We hypothesized that toe pressure in the standing position, which is close to the actual movement, may be a gait speed-related function. This is because kicking off while pressing down on the floor with the toes is necessary for walking. However, no reports have clarified the association between maximum walking speed and toe pressure strength in the standing position in older adults with disabilities.
Therefore, we examined the association between the maximum walking speed and toe pressure strength in the standing position. We believe that this study will assist in the creation of rehabilitation programs aimed at improving walking speed in older adults. Furthermore, we aimed to demonstrate the significance of assessing toe pressure in the standing position in older adults.
MATERIALS AND METHODS
Participants
This cross-sectional study included healthy residents aged ≥65 years who participated in physical fitness tests conducted at community centers and who were not hospitalized due to illness or certified as long-term care residents, as well as older adults certified as requiring long-term care undergoing physical fitness tests at daycare rehabilitation centers. Participant recruitment was performed by posting on a website, distributing flyers, and calling participants by staff members who conducted the physical fitness test. The exclusion criteria were individuals who needed assistance in walking, had deficiencies in the assessment items, and were aged ≤64 years.
The participants were fully informed of the study content and purpose and their cooperation was sought after gaining their understanding. Participation in this study was voluntary, and non-participation or withdrawal during the study was not detrimental. Additionally, before starting this study, we obtained permission from the director and site manager of the facility where the study was conducted. This study was approved by the Ethical Review Committee of Nishikyushu University (No. 210077). All participants provided informed consent. Also, this study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.15)
Measurements
We measured basic participant information including sex, age, height, weight, body mass index, and level of long-term care. The required level of care is certified by the Japanese government through the long-term care insurance certification system. In Japan, the long-term care insurance system was introduced in response to the accelerated aging of the population and accompanying increases in the level of long-term care.16) This system consists of two levels, support and care, and is further classified into seven levels: support 1–2 and care 1–5.17) We also obtained the main comorbidities of the participants from their medical records. We measured physical functions including toe pressure strength in the standing position, handgrip strength, knee extension strength, and maximum walking speed. Cognitive function was assessed using the Mini-Mental State Examination (MMSE).
Toe pressure strength in the standing position
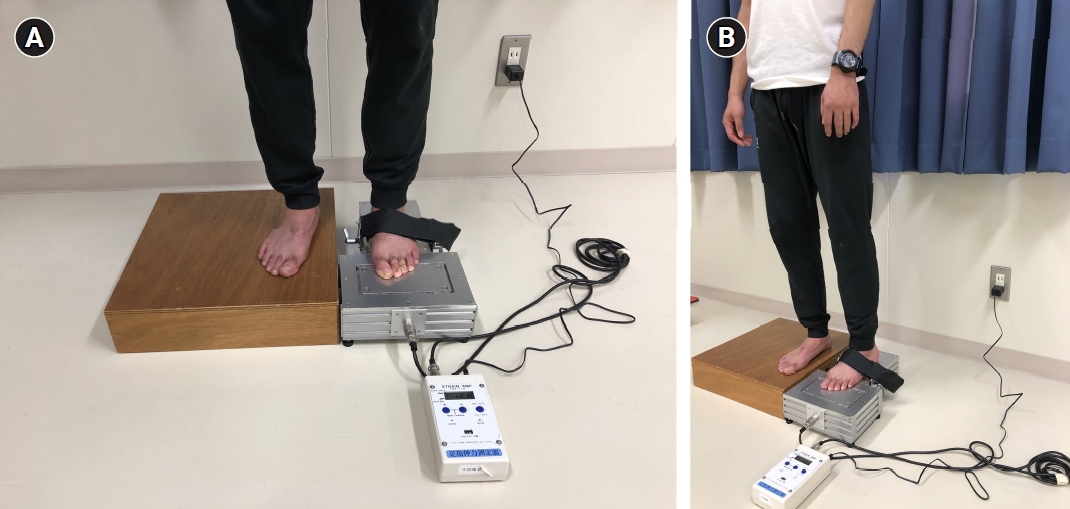
We measured toe pressure strength in the standing position using a toe pressure measuring device (S-14030; Takei Scientific Instruments Co. Ltd., Niigata, Japan). The measurement was made by securing the participant’s ankle joint with a belt, with the arms hanging loosely, and asking the participants to look straight ahead. The use of handrails or similar aids was not permitted during the measurements. To ensure accurate results, only the tips of the toes from the first to fourth metatarsophalangeal joints were placed on the force plate, and any strength of the ankle joint plantar flexion muscle was excluded from the measurement. The participants were instructed to keep their heels in place and apply force to the floor using only their toes. At the time of measurement, the subtalar joint of the foot was fixed in an intermediate position. Toe pressure was applied to the floor for 5 seconds, and the participants were permitted to adjust their weight while applying the force. As per the specifications of the device, the measured values only increase if a vertical force is applied to the force plate using the toes and not simply by shifting the center of gravity forward. Measurements were taken twice on each side. We recorded the toe pressure strength in the standing position as the sum of the maximum values on the left and right sides divided by the body weight (Fig. 1).
Other measurements
We measured handgrip strength using a Smedley-type digital grip strength meter (TKK 5401; Takei Scientific Instruments, Niigata, Japan). While standing, the participants were instructed to straighten their elbow joint and position the proximal interphalangeal joint of their index finger at a 90° angle. The evaluator ensured that the upper limbs did not contact the lower limbs or torso during the measurements. Measurements were taken twice, alternating left and right, and the sum of the left and right values was divided by body weight to obtain the handgrip strength.
We measured knee extension strength using a handheld dynamometer (μTasF-1; Anima Co. Ltd., Tokyo, Japan) with the participants sitting with their trunk upright and arms crossed over the chest. The sensor was attached to the lower leg near the ankle with a belt. Measurements were taken twice, alternating left and right, and the sum of the left and right values was divided by the body weight to obtain the knee extension strength.18)
We measured the maximum walking speed using a digital stopwatch. We instructed the participants to walk 11 m on a flat surface at a brisk pace and recorded the time it took to cover the middle 5-m section. The test was performed twice, and the fastest walking speed was recorded.
MMSE was assessed face-to-face using a questionnaire. The MMSE is the most commonly used brief cognitive assessment tool, with demonstrated reliability and validity.19) We used the MMSE in this study to ascertain how the participants understood the instructions given during the measurements.
Statistical Analysis
We initially performed Pearson correlation analysis for the measures hypothesized to correlate with maximum walking speed. The effect size (ES) was determined according to the r value—small (ES≤0.1), medium (0.1<ES≤0.3), and large (ES>0.5).
We performed a regression analysis with the maximum walking speed and toe pressure strength in the standing position as dependent and independent variables, respectively. Additionally, Model 2 was created, which included knee extension strength, sex, age, height, and level of long-term care required as covariates. We confirmed the validity of the regression equation using analysis of variance (ANOVA) and determined the goodness-of-fit of the multiple regression equation using the R2 value. We determined the multicollinearity of the multiple regression equation based on the variance inflation factor (VIF).
We used a two-tailed test to calculate the sample size for the correlation analysis using the following parameters ES (r)=0.3, α error=0.05, and power=0.8, which indicated that 82 participants were required. The number of samples required for multiple regression analysis was calculated as follows: ES (f2)=0.15, α error=0.05, and power=0.8, thereby requiring six independent variables. Therefore, this study included a total of 98 participants. The statistical significance level was set at 5%, and we used IBM SPSS Statistics for Windows, version 28.0 (IBM Corp, Armonk, NY, USA) for the analyses. G*Power 3.1.9.7 was used for sample size calculation.
RESULTS
Participant Selection Criteria
The participant selection process is detailed in Fig. 2. This study included 239 participants who completed the physical fitness test. We excluded 3, 53, and 33 participants who needed assistance with walking, had missing assessment items, and were <64 years of age, respectively. After excluding these 89 participants who met the exclusion criteria, the analysis included 150 community-dwelling older adults (81±8 years, 73% female) who participated in the physical fitness test (Fig. 2). The participants’ characteristics are shown in Table 1.
Correlation Analysis of Each Measured Item
Table 2 presents the results of the correlation analyses. These results showed a significant positive correlation between the maximum walking speed and toe pressure strength in the standing position, indicating moderate ES (r=0.48, p<0.001). Furthermore, maximum walking speed was significantly positively correlated with handgrip strength (r=0.57, p<0.001), knee extension strength (r=0.67, p<0.001), and height (r=0.23, p=0.005) and negatively correlated with age (r=−0.52, p<0.001). Moreover, toe pressure strength in the standing position was positively correlated with handgrip strength (r=0.55, p<0.001), knee extension strength (r=0.61, p<0.001), and age (r=0.20, p=0.020).
Association between Maximum Walking Speed and Toe Pressure Strength in the Standing Position
Table 3 also presents the results of the regression analyses. First, we performed a single regression analysis with the maximum walking speed and toe pressure strength in the standing position as the dependent and independent variables, respectively. The results revealed a significant association of maximum walking speed with toe pressure strength in the standing position (standardization factor=0.48, p<0.001). The results of the multiple regression analysis with knee extension strength, sex, age, height, and level of long-term care as covariates demonstrated the association of maximum walking speed with toe pressure strength in the standing position in Model 2 (standardization factor=0.13, p<0.026). The results of the ANOVA for Model 2 were significant (p<0.001), with an R2 value of 0.74. No variables with VIF >5 were identified.
DISCUSSION
In this study, we examined the association between toe pressure strength in the standing position, which is similar to the actual movement, and maximum walking speed in older adults, including those who were certified as requiring long-term care. Furthermore, we examined the association between maximum walking speed and toe pressure strength in the standing position, even after introducing variables potentially associated with maximum walking speed in older adults.
First, we examined the correlation between the maximum walking speed and each of the measures through Pearson correlation analysis. We observed a significant correlation between maximum walking speed and toe pressure strength in the standing position. We also observed a moderate effect. In other words, the stronger the toe pressure strength in the standing position, the faster the maximum walking speed. This result was consistent with our hypothesis. A previous study on young participants showed a correlation between the toe muscle strength measured by toe grip strength and walking speed.20) We observed results similar to those shown in previous studies for toe pressure strength in the standing position, which is close to the actual movement. To increase walking efficiency, the foot should be stiffer and exert a more effective force to push against the ground.21) One mechanism that increases foot stiffness is the windlass mechanism, wherein the medial longitudinal arch is elevated by toe extension, thereby improving the energy efficiency between the foot and the ground.22) Therefore, to increase walking efficiency, the toes should be pressed against the ground without flexion. This supports the possibility that the toe pressure strength in the standing position is more important than toe grip strength, which is measured by toe flexion.
The results of the regression analysis showed that toe pressure strength in the standing position was significantly associated with the maximum walking speed as the dependent variable. Multiple regression analysis in Model 2, which was adjusted for covariates, also showed a significant association between maximum walking speed and toe pressure strength in the standing position. Interestingly, toe pressure strength in the standing position was associated with gait speed in older adults even when factors already associated with gait speed were introduced. This finding indicated that toe pressure strength in the standing position contributes to maximum walking speed in older adults. Toe muscle strength may contribute to the motion that accelerates the center of gravity in the terminal stance during walking.23) In this stance, approximately 20%–30% of the body weight is applied to the toes24) and the toes perform the important movement of kicking while supporting the body weight. Therefore, because the body weight must be supported with the toes while kicking off the floor to generate propulsive force during walking, we speculate an association between maximum walking speed and toe pressure strength in the standing position. Previous studies on maximum walking speed identified toe muscle strength as a factor affecting propulsive force during walking.25) Therefore, we defined maximum walking speed as the dependent variable in this study. Interestingly, older adults have reported increased pressure on all toes when conditioned to walk at maximum speed.26) These results support the significance of evaluating toe pressure strength in the standing position, which is closer to the actual movement than toe grip strength in the sitting position. In addition, during walking, the center of pressure (COP) shifts from the heel toward the big toe. We previously showed that toe pressure strength in the standing position may contribute more to the forward shift of the COP than toe grip strength.27) Our previous findings support the present findings that gait with the forward movement of the COP is associated with toe pressure strength in the standing position, as well as our speculation that toe pressure strength in the standing position is more strongly associated with gait speed in older adults than toe grip strength.
A strength of this study is its novel determination of the association between toe pressure strength in the standing position and maximum walking speed in older adults. The results of our study of older adults, including those certified as requiring long-term care, demonstrated the need to measure toe pressure in the standing position, in addition to other physical functions, in assessing the reduction of maximum walking speed.
This study has several limitations. First, we did not measure toe grip strength; therefore, we could not compare this value with toe pressure strength in the standing position. However, a previous study examining the association between toe grip strength and maximum walking speed reported a correlation coefficient (r) of 0.42.28) Determining which is more correlated is impossible; however, a comparison of the correlation coefficients suggested similar or better correlations. Additional studies are needed to determine which toe evaluation is more relevant to the maximum walking speed by performing simultaneous measurements. Furthermore, additional studies are also needed to perform more accurate measurements of muscle strength through further validation of methods that consider toe and foot morphology. Second, while we examined the association between the maximum walking speed and toe pressure strength in the standing position, we did not measure gait parameters in detail. Previous reports indicate that older adults increase their cadence but not their stride length when increasing their walking speed.29) Therefore, detailed gait parameters should be considered in future studies. Third, we considered a small number of variables. Therefore, additional studies are needed to comprehensively incorporate and analyze the variables potentially related to walking speed. Finally, the cross-sectional study design prevented the identification of causal relationships. Therefore, future longitudinal studies are needed. However, considering concerns regarding toe grip strength in the sitting position, we clarified the significance of measuring toe pressure strength in the standing position, which is closer to the actual movement. We believe that our study results will contribute to future rehabilitation of older adults.
In conclusion, the results of this study demonstrated the positive correlation between toe pressure strength in the standing position and maximum walking speed in older adults. Moreover, toe pressure strength in the standing position was associated with maximum walking speed. Our results suggest that assessing toe pressure strength in the standing position may be used to help older adults maintain and improve their maximum walking speed, which plays a significant role in activities of daily living. Furthermore, we demonstrated the significance of evaluating toe pressure strength in the standing position.