INTRODUCTION
Aging results in a decline in the quantity and quality of human skeletal muscle, a condition known as sarcopenia.1) Sarcopenia significantly affects the quality of life and independence of elderly adults by limiting their ability to perform daily functional activities such as standing up from a chair and walking, as well as increasing the risk of falls in this population.2,3) Ultrasound imaging is a noninvasive and safe method that can be used to assess skeletal muscle quality. Among these qualities, echo intensity (EI) is an important indicator of the proportion of noncontractile elements during aging. EI reflects the infiltration of fatty and fibrous tissue of the muscle and is quantified by examining the darkness of interest in selected areas, in which black and white indicate high and low muscle quality, respectively.4,5) The loss in muscle strength associated with skeletal muscle wastage and sarcopenia may arise from decreased muscle quality, with lower extremity strength declining more markedly than that of the upper extremities during aging, ranging from 10% to 15% loss of leg strength per decade until the age of 70 years, followed by a more rapid loss, ranging from 25% to 40% per decade.6,7)
Previous cross-sectional studies have reported significant associations between muscle quality measured using EI in the lower extremities of older adults. For instance, EI transverse images of older subjects were correlated with knee extension isometric strength (r=-0.40),8) isometric strength (r=-0.62),9) and rate of force/torque development (r=-0.39).10) In addition, quadriceps EI was negatively correlated with handgrip strength in older adults (r=-0.386).11) Interestingly, the connection of EI with muscle strength is independent of endurance and muscle size.8,9) Meanwhile, evidence has shown an inverse relationship between adiposity-to-muscle ratio assessed by ultrasound EI and functional performance in older adults, with lower EI values associated with better performance. EI is also the strongest predictor of the 30-second sit-to-stand test (30SS) (r=-0.56).12) Furthermore, EI is associated with gait-related performance, considering the role of the lower extremity muscles in locomotion. The EI of the vastus lateralis was weakly correlated with usual gait speed (USG; r=-0.05) and maximal gait speed (MGS; r=-0.11),13) while a moderate correlation was reported between the EI of the rectus femoris and USG (r=-0.46).14)
Although the available data indicate that the infiltration of noncontractile elements may affect muscle strength and functional performance in older individuals, no meta-analysis has explored the correlation between lateral EI images and muscle strength or physical function in this population. Therefore, this systematic meta-analysis investigated the associations among EI (representing muscle quality), muscle strength, and physical function in older individuals.
MATERIALS AND METHODS
We conducted this review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.15) The PROSPERO International Prospective Register of Systematic Reviews (CRD42023387441) registered the review protocol, to which we adhered without any deviations.
Search Strategy
We employed a systematic search strategy using Boolean operators in the PubMed, Embase, Web of Science, SPORTDiscus, and CINAHL databases through October 2022. We modified the keywords and Boolean operators according to each database's search strategy and restricted the search to studies involving humans, written in English, and reported in peer-reviewed journals. The search strategy is presented in Supplementary Table S1.
Selection Criteria
Studies meeting the following criteria were included: (1) healthy community residents aged ≥60 years without major neurological and musculoskeletal disorders; (2) muscle mass testing using EI and reporting at least one direct assessment of muscle strength or physical function performance; (3) observational studies, including cross-sectional studies, cohort studies, and a few case-control studies; (4) published studies in English.
Articles were excluded if (1) the participants were currently on medication or had an injury that limited their physical activity and independence in daily living; (2) the study was conducted in an animal model; (3) the participants received interventions other than usual care or placebo, or randomized controlled trials; (4) the results were partially unable to extract the correlation coefficient; (5) reviews, abstracts, case reports, or duplicate published articles; and (6) non-English articles.
Two independent researchers screened the titles and abstracts of all studies based on the inclusion and exclusion criteria and then reviewed the full text of the remaining studies. Disagreements were resolved through discussion.
Data Extraction
The data extraction process involved coding the author information, publication year, and population characteristics (sample size, sex, and mean age). The correlation coefficient (r) or standardized beta coefficient between EI and two continuous muscle strength or physical function variables was extracted. The test modality/results and the results of the muscle strength assessments and physical function tests were also coded. Muscle strength was categorized into lower extremity maximum strength (i.e., maximal voluntary force/torque of the force-/torque-time curve [MVC]), explosive force (i.e., rate of force/torque development [RFD/RTD]), and handgrip strength (assessed with a handheld dynamometer [HGS]), while physical function was divided into gait speed and mobility. Gait speed (e.g., UGS and maximum gait speed [MGS]), chair stand test (e.g., 30SS), five repetitions of the sit-to-stand test (5STS), and Timed Up-and-Go (TUG) test were used to classify physical function. If no correlation was reported, the authors were contacted for the missing information. If the author did not respond, the study was excluded from the analysis.
Data Quality
We assessed the risk of bias in the included studies using the Joanna Briggs Institute Analytic Cross-sectional Study Quality Checklist (Supplementary Table S2). We evaluated the methodological quality of the selected studies according to eight items that assessed the inclusion criteria, study participants and settings, criteria for condition measurement, validity and reliability of exposure and outcome measures, confounding factors and resolution strategies, and statistical analysis. Two authors evaluated each item, which was rated as “yes,” “no,” “unclear,” or “not applicable.”
Statistical Analysis
We conducted the meta-analysis using Comprehensive Meta-Analysis (CMA), version 3.3.070, to analyze the Pearson product-moment correlation coefficients (r) obtained from the included studies. The r-values were converted into normally distributed variables (z-transformed Rz-values) using Fisher z-transformation according to the following formula16):
where ln is the natural logarithm.
We converted the beta coefficient (β) to an r value using the following formula17):
We calculated the weights of the studies based on standard errors (SE) using the following formula:
where N is the sample size.
We selected a random-effects model for the meta-analysis.
Correlations (positive or negative) were classified as small (r<0.3), medium (0.3≤r≤0.5), or large (r>0.5).18) We generated forest plots to display studies with 95% confidence intervals (CI) and the combined coefficients. The Rz values were reverse-converted to r values to classify and interpret relevant sizes. We evaluated the heterogeneity of the results between studies using the I2 index, where I2≤25% indicated low heterogeneity, I2>25% and I2<75% indicated moderate heterogeneity, and I2≥75% indicated high heterogeneity.19) Finally, we used funnel plots to investigate the possibility of publication bias.
RESULTS
Search Characteristics
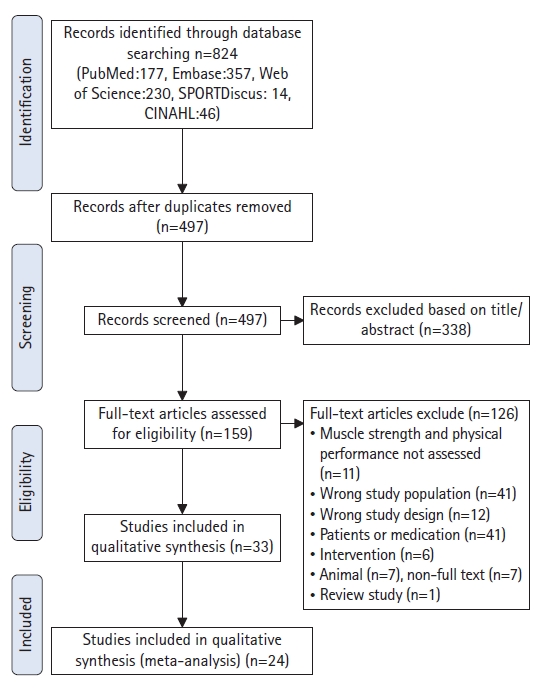
A total of 824 articles were retrieved from the initial database search through October 2022. After removing duplicates (n=327) and 338 articles based on the title or abstract, 159 articles remained and were assessed for eligibility. Finally, 24 articles were included in the meta-analysis (Fig. 1). A total of 2,501 people were included in this review, and the mean age was 71.3±5.5 years. The sample sizes ranged from 12 to 1,239. Supplementary Table S3 details the baseline characteristics of the included studies.
Association between EI and Muscle Strength
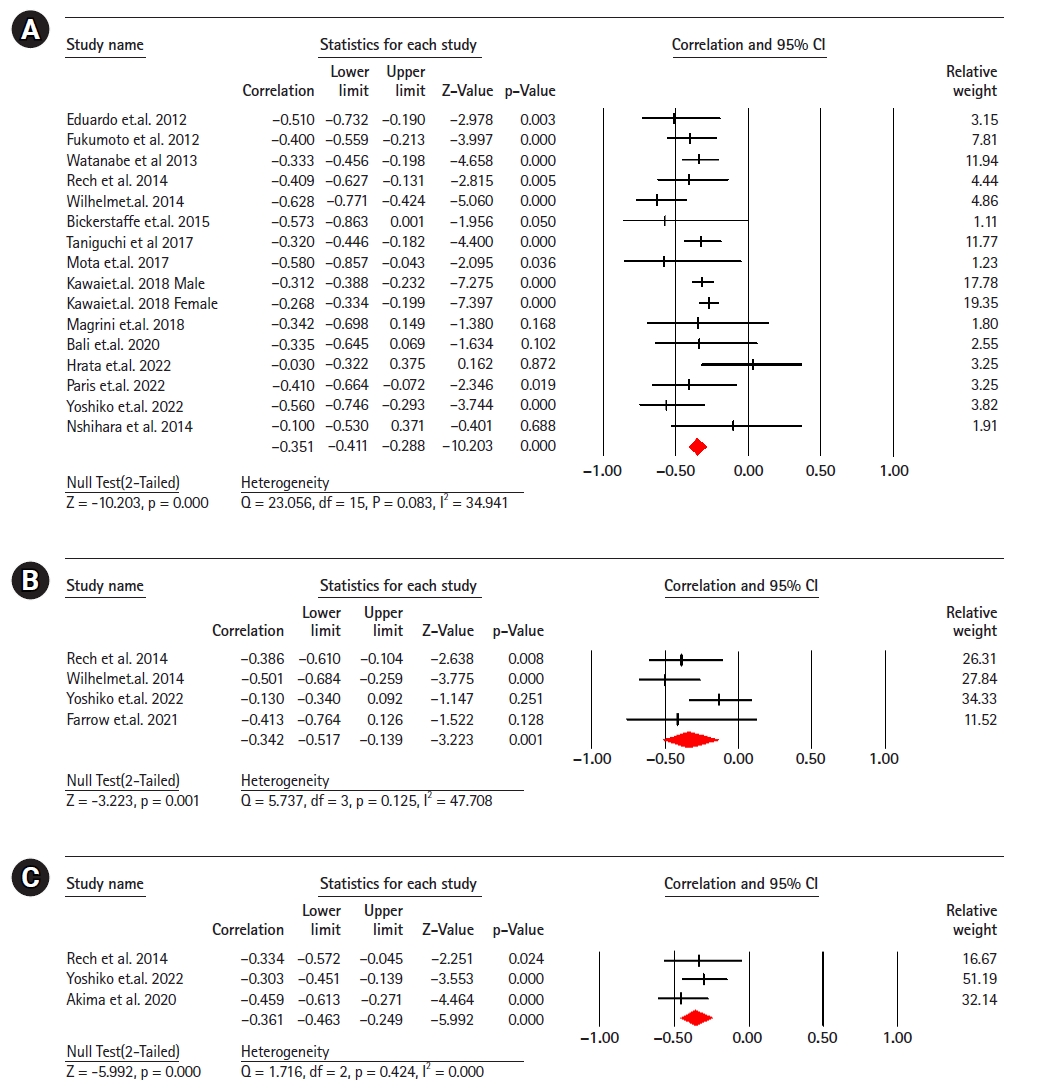
Sixteen studies (2,009 participants) analyzed the association between EI and maximal strength in healthy older adults.8,9,11,13,20-30) The results revealed a significant moderate correlation negative between EI and maximum strength (r=-0.35; 95% CI, -0.41 to -0.28; p<0.001; I2=34.94). Four studies (190 participants) analyzing the association between EI and explosive power in healthy older adults,11,22,28,31) showed a significant moderate negative correlation between EI and explosive power (r=-0.34; 95% CI, -0.51 to -0.13; p=0.001; I2=47.70). Three studies (261 participants) showed a moderate negative correlation between EI and handgrip strength11,32,33) (r=-0.36; 95% CI, -0.46 to -0.24; p<0.001; I2=0.000) (Fig. 2).
Association between EI and Physical Function
Gait speed
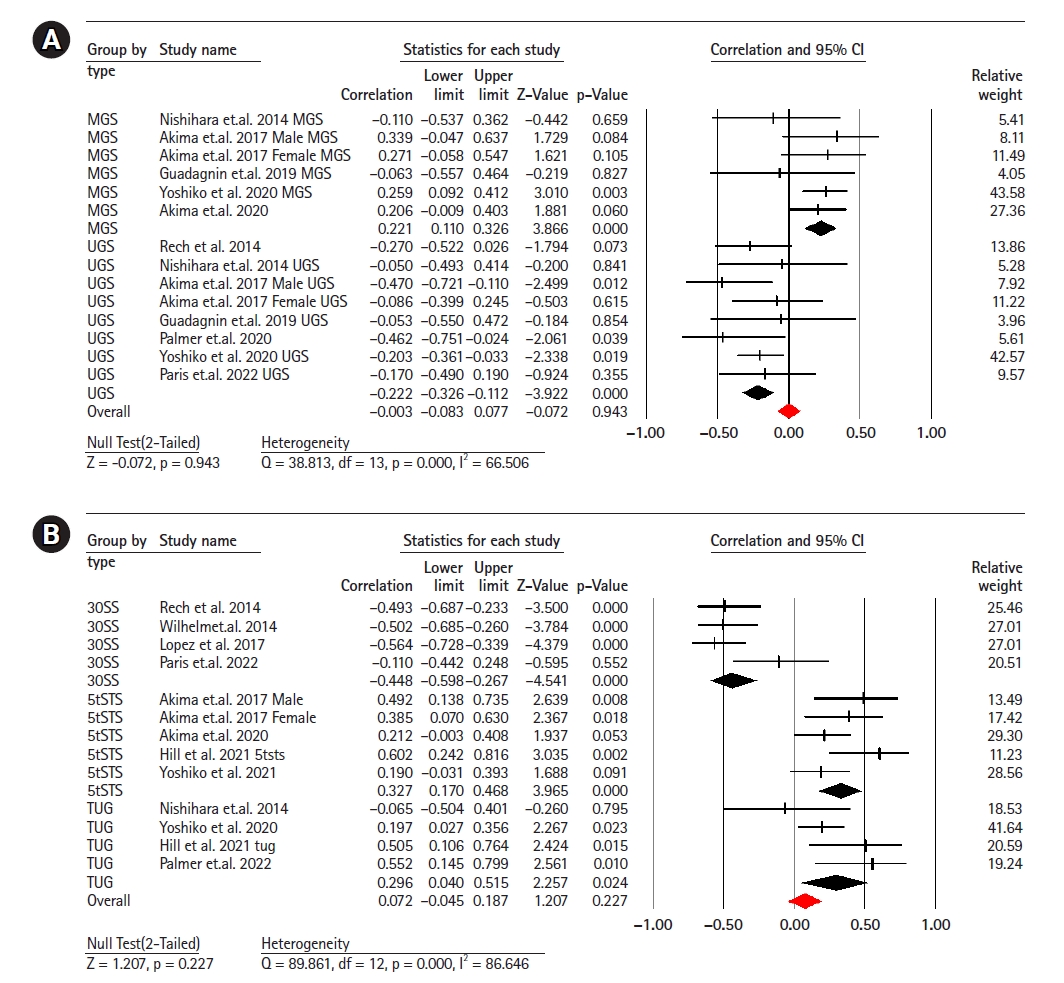
Fourteen studies (involving 641 participants) investigated the association between EI and gait speed.11,13,14,21,22,33-35) The combined effect size for EI and gait speed was r=0.00 (95% CI, -0.08 to -0.07; p=0.94; I2=66.50), indicating no linear correlation between the two with moderate heterogeneity. Subgroup analysis showed a weak negative correlation between UGS and EI (r=-0.22; 95% CI, -0.32 to -0.11; p<0.001; I2=0.00), while there was a weak positive correlation between MGS and EI (r=0.22; 95% CI, 0.11 to 0.32; p<0.001; I2=0.00) (Fig. 3).
Chair stand test
Thirteen studies (620 participants) investigated the association between EI and the chair stand test.11-14,21,29,32,35-37) The combined effect size of EI and 30SS was r=0.07 (95% CI, -0.04 to 0.18; p=0.22; I2=86.64), with a weak statistical correlation and considerable heterogeneity. Subgroup analyses showed a moderate negative correlation between EI and the 30SS test (r=-0.44; 95% CI, -0.59 to -0.26; p<0.001; I2=45.41) and between EI and the 5STS test (r=0.32; 95% CI, 0.17 to 0.46; p<0.001; I2=35.42), respectively. We observed a weak positive correlation between EI and the TUG test (r=0.29; 95% CI, 0.04 to 0.21; p=0.02; I2=25.42) (Fig. 3).
Publication Bias
The relative symmetry displayed in Fig. 3A indicates no apparent publication bias. Visual inspection of the funnel plot in Fig. 3B suggested insufficient evidence of publication bias, with an intercept result of 1.03 (SE=2.10; 95% CI, -3.51 to 5.58; t=0.48; df=13; p=0.63), indicating no strong evidence of publication bias (Supplementary Fig. S1).
DISCUSSION
This meta-analysis examined the correlation between EI in the thigh muscles, muscle strength, and physical functional performance in healthy older individuals.
Our results revealed a significant moderate inverse correlation between EI and maximal strength in the lower extremities, explosive power, and handgrip strength in this population. However, the meta-analysis showed contradictory evidence for the association between EI and physical functional performance, which appeared to be task-specific. In summary, the strength of the association between thigh EI and physical function may depend on the specific type of physical function test used.
Correlation between Muscle Strength and EI
The results of our meta-analysis suggested a moderately negative correlation between EI and muscle strength in older adults. Muscle quality, which is related to the amounts of muscle fiber and fat tissue, is an independent determinant of muscle strength. Gray-scale analysis of EI is a valuable tool for assessing muscle strength.5) Furthermore, the relationships between EI and different types of strength exhibit unique features. EI and maximum strength are negatively correlated (r=-0.3), with the fat and connective tissue in muscles playing a significant role in isometric and isokinetic strength in older adults. This finding is consistent with those of previous studies showing a correlation between the EI of the rectus femoris muscle and isometric/isokinetic peak torque, with r values ranging from -0.40 to -0.67.8,30) However, contrary to our study, these previous studies observed no relationship between thigh EI and maximal isometric strength.38) One explanation for this discrepancy could be the use of different measurement techniques to assess EI. In EI determined from transverse images, the ultrasound probe positioning significantly affects the results.5) Therefore, discrepant findings in the literature may be due to differences in probe orientation. The current evidence suggests that the accumulation of non-contractile components in thigh muscles significantly affects maximal knee extension and flexion strength in older adults.28)
A previous study showed that older adults experience a more significant decline in explosive speed than in maximum muscle velocity.39) Our results demonstrated a moderate correlation (r=-0.3) between EI and knee explosive power, which can be attributed to the increased intramuscular fat infiltration associated with aging. This change leads to a decrease in single-fiber contraction velocity and power output, alters mechanical muscle properties, increases muscle stiffness, and alters fiber shortening and bulging.8,40) Additional neuromuscular variables contribute to the age-related decrease in explosive speed; specifically, the fast performance of older adults may be influenced by motor unit firing rate.41) In addition, the decline in muscle strength associated with aging may be owing to factors beyond muscle mass, such as decreased proportion of fast type II fibers and reduced muscle excitatory neural activation.42-44) Moreover, coactivation, which refers to opposing muscle mechanical action, is higher in older adults, resulting in reduced force production.45)
The assessment of grip strength using a HGS is a practical approach for evaluating muscle strength in clinical contexts.46) In addition to its ease of application, grip strength can serve as a crucial indicator of physical functionality and is associated with mortality rates in certain pathological conditions. Our meta-analysis identified a moderate correlation (r=-0.3) between EI strength and handgrip strength, consistent with the outcomes of various previous studies.11,32,33)
Correlation between Physical Function and EI
Although we did not observe a significant association between EI and gait speed, subgroup analyses revealed a weak association between maximal and usual gait speeds. Previous research on older adults showed no significant correlation between the muscle EI of the quadriceps femoris and the 6-minute walk, which was attributed to an increase in subcutaneous fat thickness. However, the relationship became statistically significant after adjusting for subcutaneous fat.34) These findings raise concerns about whether it is necessary to adjust for subcutaneous fat thickness in EI measurements for older adults.
We examined the relationship between chair-stand performance and EI. We observed a weak correlation between chair-stand performance and EI, with substantial heterogeneity. Previous studies comparing various types of chair tests have reported that a 30-second chair stand is the optimal parameter for predicting EI in older adults.36) Subgroup analysis revealed a moderate correlation (r=0.4) between 30-second chair stand performance and EI, supporting the previous finding that an increased proportion of non-contractile elements may lead to functional status deterioration with aging.4) The high heterogeneity in the meta-analysis may have resulted from using different cutoff points. Age is a primary factor affecting chair-stand performance and EI and may confound the assessment of this association. Moreover, ankle plantar flexors exhibit a similarly strong association (r=0.45–0.59) with chair function tests in older adults,37) implying that muscle type may account for the lack of significant association between chair-stand tests and EI in our study.
In addition, EI obtained using ultrasound may be influenced by methodological factors such as subcutaneous fat correction, biological factors such as sex and race, and environmental factors such as daily physical activity and exercise,5,47,48) which cannot be completely controlled in clinical settings. The inconsistency between the results of our meta-analysis and those of previous studies emphasizes the need to carefully consider confounding factors when examining the relationship between EI and physical function.
This study had several limitations. First, due to the lack of a standardized EI measurement method, we used raw EI data. Subcutaneous fat thickness may attenuate ultrasound findings and affect the reliability of muscle EI results. Second, insufficient data were available to perform a meta-analysis of muscles outside the thigh; therefore, the analysis does not represent the strength and overall function of the lower limb muscles. In addition, not all the studies controlled for confounding variables. Although this report examined the results in older adults, the included studies did not separately investigate participants by sex; therefore, potential differences between the sexes are unknown. Finally, the current meta-analysis was based on cross-sectional data; thus, the association does not imply causality. Therefore, the relationship between muscle structural characteristics, muscle strength, and physical function variables could not be determined.
Overall, our meta-analysis results support EI as an effective indicator for evaluating muscle strength and physical functional performance; however, the influence of factors such as different muscle types, age, and sex must be considered. Future research should explore the impact of these factors on this relationship to better understand the application of echogenicity in evaluating muscle strength and functional performance.
Conclusion
Our findings suggest that increased EI in the thigh muscles is associated with decreased strength and power in older individuals. However, we did not observe a significant association between EI and gait speed or mobility. Further well-designed studies with larger sample sizes and longer-term follow-ups are required to validate the practical implications of these results in predicting frailty and assessing risks in this population.