Association of Vulnerability Screening on Hospital Admission with Discharge to Rehabilitation-Oriented Care after Acute Hospital Stay
Article information

Abstract
Background
The short Dutch Safety Management Screening (DSMS) is applied at hospital admission of all patients aged >70 years to assess vulnerability. Screening of four geriatric domains aims to prevent adverse outcomes and may support targeted discharge planning for post-acute care. We explored whether the DSMS criteria for acutely admitted patients were associated with rehabilitation-oriented care needs.
Methods
This retrospective cohort study included community-dwelling patients aged ≥70 years acutely admitted to a tertiary hospital. We recorded patient demographics, morbidity, functional status, malnutrition, fall risk, and delirium and used descriptive analysis to calculate the risks by comparing the discharge destination groups.
Results
Among 491 hospital discharges, 349 patients (71.1%) returned home, 60 (12.2%) were referred for geriatric rehabilitation, and 82 (16.7%) to other inpatient post-acute care. Non-home referrals increased with age from 21% (70–80 years) to 61% (>90 years). A surgical diagnosis (odds ratio [OR]=4.92; 95% confidence interval [CI], 2.03–11.95), functional decline represented by Katz-activities of daily living positive screening (OR=3.79; 95% CI, 1.76–8.14), and positive fall risk (OR=2.87; 95% CI, 1.31–6.30) were associated with non-home discharge. The Charlson Comorbidity Index did not differ significantly between the groups.
Conclusion
Admission diagnosis and vulnerability screening outcomes were associated with discharge to rehabilitation-oriented care in patients >70 years of age. The usual care data from DSMS vulnerability screening can raise awareness of discharge complexity and provide opportunities to support timely and personalized transitional care.
INTRODUCTION
A growing number of older hospital patients can benefit from rehabilitation-oriented post-acute care (PAC) to improve their functional outcomes after hospital discharge.1,2) However, age is not an identifying criterion for referral for geriatric rehabilitation. Rather, multidisciplinary assessments and geriatric expertise must establish a genuine need for geriatric rehabilitation in older or more vulnerable hospital patients.3,4) These PAC decisions extend across healthcare settings and are professionally and managerially challenging for hospital teams.5-9)
To support PAC decision-making and enhance the coordination of services following discharge from the hospital, discharge planning should preferably start from admission by following candidates for PAC.10-12) Patient characteristics such as older age, female sex, frailty, lower functional or cognitive status at admission, comorbidities, and length of hospital stay are associated with the development of rehabilitation needs and functional impairments during hospital stays.13-15) To prevent functional decline in vulnerable patients and other adverse outcomes such as institutionalization, various vulnerability screening instruments have been developed.16-18) The vulnerability score of the mandatory Dutch Safety Management System (DSMS) was introduced in Dutch hospitals in 2012 and has been applied to all patients aged >70 years at admission. The DSMS tool consists of short screening instruments in four geriatric domains: delirium, functional impairment, malnutrition, and fall risk.19-22)
Early identification of vulnerable older patients at hospital admission aims to diminish the risk of functional decline during the hospital stay through targeted in-hospital geriatric interventions. Subsequently, early and repeated assessments of rehabilitation needs, exploration of individual motivation, and establishment of an individual prognosis for recovery may identify candidates for geriatric rehabilitation early during their hospital stay and enhance personalized PAC decision-making.11,12) Although the mandatory DSMS screening of seniors at hospital admission was not designed nor validated to identify patients to undergo rehabilitation, an association could exist between the “risk of adverse outcome profile” in these patients and the appropriateness of rehabilitation-oriented care at discharge. Early profiling of potential geriatric rehabilitation candidates using available demographic and clinical admission data, including vulnerability scores, may allow for early decision-making concerning rehabilitation-oriented PAC. We hypothesized that DSMS vulnerability scores would differ between patients referred for geriatric rehabilitation and those discharged home. Therefore, we sought to identify patient characteristics related to the DSMS screening domains that were associated with referral to rehabilitation-oriented care after an acute hospital stay.
MATERIALS AND METHODS
Setting and Design
Amsterdam University Medical Centers is a large (1,700-bed) tertiary academic medical center with two facilities. Both hospitals are situated in an urban health region and provide specialized medical care to a large, predominantly urbanized region. One hospital has a geriatric rehabilitation unit. Skilled nursing facilities, nursing homes, and private care organizations in the area provide rehabilitation-oriented PAC consisting of geriatric rehabilitation and short-stay residential care. Short-stay residential care is indicated when older patients require temporary nursing home care for recovery.23) We undertook a retrospective cohort study of community-dwelling patients aged >70 years who were discharged from the hospital between January 15 and May 15, 2019.
Patients
This study included hospital episodes of community-dwelling patients aged >70 years discharged after acute admission from a single facility. Acute admission was defined as an admission following emergency room admission. The minimum hospital stay was one night. If a patient was admitted more than once during the study period, we included the last hospital episode following the acute admission. We excluded admitted patients who had died and those discharged from other hospitals, and included patients discharged to the in-hospital geriatric rehabilitation unit. Three subgroups of patients were formed according to discharge destination: home, geriatric rehabilitation, and other PAC in a nursing home. Usual care data were extracted from the patients’ medical records. The demographic variables included age, sex, place of residence before admission, and discharge disposition (home, nursing home, or other hospital). Data on the living conditions were not available. Clinical data included attending medical specialty; admission diagnosis; comorbidities; and DSMS data on functional status, nutritional status, falling risk, and presence of delirium symptoms. We collected DSMS data within 48 hours of admission and information concerning consultant specialists, paramedical treatment, and length of hospital stay. The discharge destination for inpatient PAC was geriatric rehabilitation or other nursing home care.
Measurement Instruments
Table 1 presents the vulnerability screening system of the DSMS. This system consists of the Simplified Nutritional Assessment Questionnaire (SNAq) for nutritional status, Katz activities of daily living (ADL) for functional status, and screening questions for delirium and falls.24-26) In the population under study, the adapted version of DSMS was used. The falling risk was assessed using the Johns Hopkins Risk of Falls Assessment Tool (JHRFAT) instead of a single question regarding the history of falls. The JHRFAT is widely used for measuring age, fall history, incontinence, medication use, use of patient-care equipment, mobility, and cognition. Scores of 6–13 and >13 points indicate moderate and severe fall risks, respectively.27,28) We used the Delirium Observation Screening Scale (DOS) to identify the confusion symptoms. The DOS comprises 13 items in seven domains (consciousness, attention, thinking, memory/orientation, psychomotor activity, mood, and perception) and is applied to the presence of delirium symptoms instead of three screening questions on the confusion symptoms. Each item of the DOS was scored during one 8-hour nursing shift (day/evening/night). A score of three or more points was considered positive.29,30)
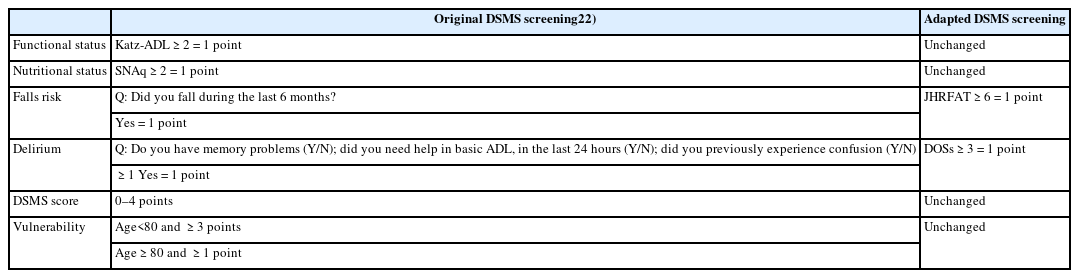
Original and adapted DSMS vulnerability screening
In the DSMS tool, the score of each separate instrument is dichotomized into the presence or absence of risk and summed to obtain the DSMS score for vulnerability, with a range of 0–4. Vulnerability is defined as DSMS scores of ≥3 and ≥1 in patients aged 70–79 and ≥80 years, respectively.17,19) Table 1 lists the components of the DSMS vulnerability score and vulnerability calculation. The age-adjusted Charlson Comorbidity Index (CCI), based on reported comorbidities, adds one point for every decade over 40 years of age.31)
Analysis
We analyzed the data using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). According to the discharge destination after the hospital stay, the data were divided into home (H), geriatric rehabilitation (GR), and other nursing home care (NH). Comorbidity data were computed using the age-adjusted CCI.32) When the Katz-ADL or JHFRAT scores were assessed more than once during the hospital stay, we analyzed the final score. Next to DOSs ≥3, the number of positive DOSs (≥3) was used as an additional variable.
Data were analyzed according to the discharge destination (H, GR, and NH). For analysis of total inpatient PAC discharge, the GR and NH groups were combined to form the “non-home group.” We performed comparisons between groups using χ2 tests for nominal data, Kruskal-Wallis tests for ordinal data, and t-tests for normally distributed continuous data. According to the original DSMS screening, the scores of the adapted DSMS were dichotomized into the presence or absence of risk to calculate the vulnerability score. We calculated the odds ratio (OR) with 95% confidence intervals (CI) of the independent variables “age,” “surgical diagnosis,” “age-adjusted CCI,” and the DSMS criteria using logistic regression analysis comparing home and non-home discharge. Bivariate correlations were evaluated (Pearson coefficient). To calculate the OR for age-adjusted CCI, we dichotomized the data according to the median value (6) in our cohort.33,34)
Ethics
The Medical Ethics Committee of the University Medical Centers Amsterdam reviewed and approved the study protocol (File No. 2018621). Also, this study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.35)
RESULTS
Fig. 1 shows a flow diagram of the study inclusion process. Among 491 total patient records included in this study, 349 (71.1%) patients were discharged H, 60 (12.2%) to GR, and 82 (16.7%) to NH. In the NH group, most (75.6%) were referred for short-stay residential care, recovery care in a nursing home for general medical needs that did not require medical specialist care, or GR.23) A minority of this group (24.4%) was referred for palliative intermediate or long-term care. Supplementary Table S1 provides an overview of the NH group.
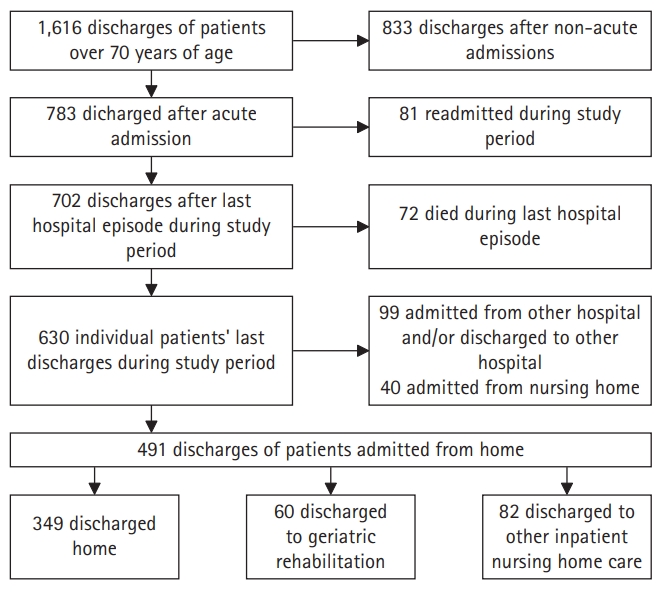
Flow diagram of inclusion.
Demographics and Comorbidities
Overall, 55.4% of the patients were male. In the H group, 59.3% were men. The sexes were evenly matched in the GH group and were 42.7% in the NH group.
In the 71–80-years age group, 79% were discharged H group, 11% to GR group, and 10% to NH group. In patients >90 years of age, 39% were discharged H group, 23% to GR group, and 38% to NH group. An overview of the data is presented in Table 2.

Demographic characteristics, referring specialism and co-morbidity in discharge destination groups
Among GR patients, 70% were acute orthopedic or trauma patients, in contrast to the H group with 12.6% surgical patients. Internal medical patients comprised 35.5% of the H group, 5.0% of the GR group, and 40.2% of the NH group. Neurological or neurosurgical patients comprised 12.9% of the H-group, 8.3% of the GR group, and 25.7% of the NH group. The mean age-adjusted CCI was 7.18 in the H group, 7.57 in the GR group, and 7.65 in the NH group (p=0.186). Overviews of the comorbidity data and main diagnoses are presented in Supplementary Tables S2 and S3.
DSMS-Vulnerability Screening
DOS scores were missing for 52% of the participants, SNAq scores in 16%, and Katz-ADL in 13%.
The JHFRAT data were complete. Symptoms of delirium (DOS ≥3) were present in 37% of the H patients, 49% of GR patients, 63% of NH patients, and 57% of all non-home discharged patients. Delirium symptoms registered on 2 or more days were present in 6% of H-group patients, 16% of GR patients, 27% of NH, and 22% of all non-home patients. Functional status was low in 28% of patients discharged home compared to 79% of GR patients, 69% of NH patients, and 73% of all non-home discharged patients. A medium or high risk of falling was observed in 52% of participants in the H-group, 73% of the GR group, 82% of the NH group, and 78% of all non-home discharged patients.
DSMS vulnerability scores were present in 30% of H group patients and 70% of NH patients. Vulnerability, according to DSMS scoring was present in 44% of H-group patients, 67% of GR patients, 75% of NH patients, and 72% of all non-home discharged patients. Table 3 presents an overview of the data. The graphs are provided in Supplementary Figs. S1 and S2.
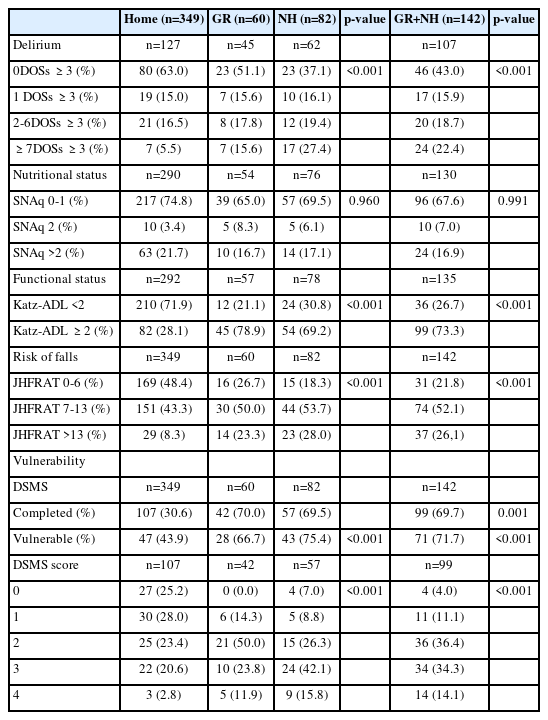
DSMS vulnerability screening of delirium symptoms (DOSs), nutritional (SNAq) and functional (Katz-ADL) status, risk of falls (JHFRAT) in discharge destination groups
Non-home Discharge
Patients with trauma or acute orthopedic needs (adjusted OR=4.92; 95% CI, 2.03–11.95) had higher odds for non-home discharge. The odds for non-home discharge were highest for patients with functional impairment, as represented by positive Katz-ADL (OR=3.79; 95% CI, 1.76–8.13) and JHFRAT scores on the risk of falling (OR=2.87; 95% CI, 1.31–6.29). We observed no associations between positive DOS (OR=2.12; 95% CI, 0.99–4.55) or SNAq screening (OR=1.64; 95% CI, 0.73–3.70) and non-home discharge. Table 4 presents an overview of the crude and adjusted ORs.
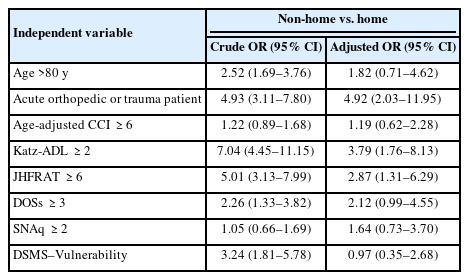
Crude and adjusted odds ratios in non-home versus home discharged patients
DISCUSSION
In this cohort of acutely admitted community-dwelling patients, two subscores of the DSMS vulnerability tool were associated with discharge to geriatric rehabilitation or other nursing home care. Usual care data on vulnerability contains valuable information for PAC decision-making. The most distinctive differences between home and non-home hospital discharge were the DSMS subscores for functional status (Katz-ADL) and falling risk (JHFRAT), both of which are multidomain measurement instruments.
DSMS Vulnerability Screening
Previous studies on the predictive properties of the DSMS vulnerability score have reported contradictory findings regarding early readmission and mortality in older hospital patients.20,21,36) No association was found between DSMS vulnerability and mortality, complications, or readmission in geriatric, cardiac, or gynecological patients.19,37-39) However, in patients with hip fractures, the DSMS vulnerability score was positively associated with mortality and a complicated rehabilitation trajectory.40,41) Moreover, low to moderate prognostic accuracy has been reported for functional decline, morbidity, hospital readmission, institutionalization, and long-term survival.19)
In a cohort of patients discharged from a geriatric ward, positive scores on all four domains of the DSMS vulnerability tool were associated with post-discharge institutionalization; however, the type of PAC was not specified.22) In our cohort of older patients discharged from all hospital wards, we observed a positive association between DSMS vulnerability sub-scores and referral to rehabilitation-oriented PAC The ORs were the highest for positive Katz-ADL (functional domain) and JHFRAT (falling risk) scores. This finding is consistent with evidence that functional metrics are significant predictors of multiple hospital outcomes, including the likelihood of discharge home and the risk of poorer functional status after acute care.42) Functional recovery and safe mobility are important geriatric rehabilitation goals. The application of DSMS screening enhances the awareness of rehabilitation needs, thus targeting potential candidates for geriatric rehabilitation at an early stage.
Non-home Discharge in Hip Fracture Patients
Most participants in the geriatric rehabilitation group in this study were patients with trauma or acute orthopedic needs and aged >80 years. As in our study, the Dutch hip fracture cohort study found that seniority, premorbid mobility problems, and premorbid Katz-ADL were independent predictors of discharge to geriatric rehabilitation vs. home.43) The original DSMS did not include a separate mobility screening; however, the JHFRAT in the adapted DSMS contains three mobility items: the need for supervision or assistance when walking, unsteady walking, and sensory loss affecting mobility. A positive JHFRAT score in our cohort had positive odds for non-home discharge (adjusted OR=2.87; 95% CI, 1.31–6.29). In the Dutch hip fracture cohort, a higher premorbid Katz-ADL score and a history of dementia distinguished between discharge to a nursing home and discharge home.43) In our study, a DOS of ≥3, which indicated the presence of delirium symptoms, did not show positive odds for non-home discharge from the hospital (OR=2.12; 95% CI, 0.99–4.55). While other studies reported that delirium in patients with hip fractures was an independent predictor of adverse outcomes, our results did not confirm this association.44-46)
Vulnerability and Discharge Decision-Making
In our cohort, a positive DSMS vulnerability score upon hospital admission indicated a certain likelihood of rehabilitation need. Being vulnerable or mildly frail does not imply the absence of rehabilitation potential.4) The identification of future geriatric rehabilitation candidates presents an opportunity to optimize in-hospital geriatric care and personalize PAC decision-making. A positive vulnerability score inspires the exploration of all factors relevant to decision-making. Comprehensive Geriatric Assessment (CGA), multidisciplinary team meetings, and the involvement of patients and families can effectively contribute to patient-centered discharge planning.47) Frailty measures such as the CGA-related frailty index may have prognostic value for rehabilitation outcomes.48,49) This frailty index, as well as the DSMS vulnerability score, can be derived from automated data and facilitates discharge decision-making by allowing the early identification of patients who may later require PAC.50)
Limitations
We analyzed the data of acutely admitted patients who were discharged from a single tertiary hospital. Both of these factors may have influenced the case mix. We assumed that the discharge of acutely admitted patients was the most representative of our research question because admission to rehabilitation-oriented PCA requires acute functional loss. This restriction and the ongoing reorganization of the two hospitals may have accounted for the change in patient flow, resulting in a high percentage of patients with trauma and a low percentage with neurological conditions in our cohort.
Our dataset has some limitations. First, due to privacy laws, data on living arrangements were not available; although living alone is an influential factor in PAC referral decisions. Second, nearly 50% of the adapted-DSMS screening data for delirium were missing. The DOS score was applied only when confusion was observed at hospital admission. The missing DOS scores explain the low percentage of completed DSMS vulnerability scores. Instructions on the application of this sub-score are important to avoid missing data. The comprehensiveness of both the DOS and JHFRAT may influence the feasibility of the DSMS.
Strengths
To our knowledge, this is the first Dutch study to address the relationship between routine vulnerability screening at hospital admission and discharge for geriatric rehabilitation. DSMS data are available in the electronic health records of all Dutch hospitals and can be used to identify potential candidates for rehabilitation-oriented PCA. These findings support hospital practices concerning geriatric treatment and facilitate the timely and careful addressing of discharge dilemmas.
As the JHRFAT in the adapted DSMS is a multidimensional “geriatric” instrument used to measure the falling risk, it may have accounted for the higher accuracy of vulnerability measurement compared to the screening question from the original DSMS.
Recommendations
DSMS vulnerability data can be used to predict discharge decisions. Timely PAC decision-making by liaison nurses, geriatricians, or rehabilitation specialists adds to the quality of transitional care. Information on living conditions and family support can further contribute to decision-making.
The inclusion of vulnerability scores in handovers can help to evaluate patient progress during rehabilitation. Frailty status may change during rehabilitation. The ADL status before hospital admission represents a parameter for goal setting in rehabilitation and supports the monitoring of functional gain.
To properly assess the association between vulnerability, appropriateness of referral decisions, and outcomes of rehabilitation-oriented PCA, we recommend a prospective cohort study with follow-up after transfer to a rehabilitation-oriented PAC.
Conclusions and Implications
DSMS vulnerability screening with a higher domain score for functional impairment and falling risk indicated higher odds for non-home discharge. Older surgical patients had the highest risk of being transferred to PCA. The usual care data of vulnerability screening at hospital admission can trigger awareness among professionals of the need for rehabilitation-oriented care at discharge, facilitating an early diligent dialogue with older patients and their families regarding preferred treatment and care after hospital discharge.
Notes
The researchers claim no conflicts of interest.
FUNDING
This research received internal funding (Internal funding from the department of Medicine for Older People, Amsterdam University Medical Center).
AUTHOR CONTRIBUTIONS
Conceptualization, RB, JW, AG, CH; Data curation, AG, JW; Methodology, JW, RB, EW; Writing-original draft, AG; Writing-review & editing, EW, RB, JW, CH.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4235/agmr.23.0068.
Post-acute care in the NH group (n=82)
Comorbidity in discharge destination groups
ICD-10 classification of main diagnosis
DSMS domain scores in non-home versus home discharged group: (A) Katz-ADL, (B) JHFRAT, (C) SNAq, and (D) DOS. DSMS, Dutch Safety Management Screening; Katz-ADL, Katz activities of daily living score (0–6); JHFRAT, Johns Hopkins Falls Risk Assessment Tool; SNAq, Short Nutrition Assessment Questionnaire (0–4); DOS, Delirium Observation Scale score (No DOS >2; 1DOS >2; 2-6DOS >2; >6DOS >2).
Distribution of DSMS scores (0–4) in non-home (n=99) and home (n=107) discharged patients. DSMS, Dutch Safety Management Screening.