Nutritional Status and Risk of Sarcopenia among Hospitalized Older Adults Residing in a Rural Region in Turkey
Article information

Abstract
Background
This study aimed to determine the prevalence of sarcopenia and its associated factors in community-dwelling older adults at risk of malnutrition based on the Mini Nutritional Assessment (MNA), Prognostic Nutritional Index (PNI), and Geriatric Nutritional Risk Index (GNRI).
Methods
The study participants were 345 adults aged >65 years who visited Geriatric Internal Medicine outpatient clinics. The study included people without acute illness for whom the risk of malnutrition could be assessed and appropriate measurements taken. At the baseline visit, participants’ data and measurements were gathered. The primary data included sociodemographic details, anthropometric measurements, malnutrition screening tests, and functional assessments.
Results
The participants’ mean age was 76.21±5.59 years, and 57.1% were men (n=97). The prevalence rate of sarcopenia was 45.5%. Compared to individuals without sarcopenia, those with it were older; had lower MNA, PNI, and GNRI scores; and had lower muscle mass, muscle strength, and lower leg circumferences (p<0.001). After adjusting for potential confounding factors, we found that sarcopenia, advanced age, male sex, high risk of malnutrition, calf circumference, and a low PNI score were all significantly associated with a low GNRI score (p<0.001).
Conclusion
Sarcopenia was significantly associated with advanced age, male sex, and high risk of malnutrition. Patients’ nutritional and functional status should always be assessed for therapeutic interventions and lifestyle changes.
INTRODUCTION
Aging is an inevitable process in which cells, organs, and entire systems change and show functional decline.1) In Turkey, people aged ≥65 years are expected to comprise 9.9% of the total population by 2022.2) As people age, they experience respiratory, cardiovascular, digestive, nervous, endocrine, immune, musculoskeletal, excretory, dermatological, ocular, otological, gustatory, and olfactory problems. Most individuals >65 years of age also have multiple chronic systemic diseases and take multiple drugs.3) Sarcopenia and malnutrition are the most common health problems and show similar physiological mechanisms in this population.4) Sarcopenia is a progressive and generalized skeletal muscle disorder involving accelerated loss of muscle mass and function and is associated with increased adverse outcomes, including falls, functional decline, frailty, and mortality.5) The European Society for Clinical Nutrition and Metabolism (ESPEN) defines malnutrition as a condition resulting from inadequate nutrient intake or an unhealthy diet, resulting in a change in body composition (lower lean mass and body cell mass), physical and mental function, and deterioration in clinical disease outcomes.6) Owing to inadequate nutrition, malnutrition develops first, triggering sarcopenia development.7,8) Thus, determining the nutritional risk, providing early treatment to slow disease progression, and ensuring the initiation of effective sarcopenia treatment in older adults are critically important. For this purpose, some nutritional screening tools and risk indices have been defined for use in older adult populations. These tools and indices are easy to apply in clinical practice, fast, low-cost, acceptable, meet high specificity and sensitivity criteria, and are suitable for continuous application.9) The Mini Nutritional Assessment (MNA) and Geriatric Nutritional Risk Index (GNRI) are among the preferred nutritional screening tools in the older adult population. MNA consists of 18 questions and is the most popular test used to assess the nutritional status of older adults. It is used to gather data on anthropometric measurements, lifestyle, food consumption, and subjective health10-12) GNRI is universally adopted to evaluate patients’ nutritional condition. It is an effective and simple risk index to present patients’ nutritional risk and has been proven to be a predictive index for prognosis in aged patients, patients on dialysis, patients with cardiovascular conditions, and in healthcare contexts.11) The Prognostic Nutritional Index (PNI) is used to determine the risk of nutrition-related complications in patients undergoing surgery.13)
The European Working Group on Sarcopenia in Older People (EWGSOP) has made several updates over the last 10 years to standardize the definition of sarcopenia. These guidelines use low muscle strength, considered the most reliable measure of muscle function, as the primary parameter for sarcopenia.14) The most common methods for evaluating muscle mass are dual-energy X-ray absorptiometry (DEXA), computed tomography, magnetic resonance imaging (MRI), bioimpedance analysis (BIA), total and partial body potassium/fat-free soft tissue ratios, and anthropometric measurements. The method used depends on cost and facilities.15) Gait speed, hand grip strength, and/or muscle mass are recommended to screen for sarcopenia starting at 65 years of age.16) The term malnutrition–sarcopenia syndrome was coined to describe the simultaneous occurrence of both malnutrition and sarcopenia, most notably in older adults, and has a higher mortality rate than that for either condition alone.17)
Older adults require adequate and nutritious food.18) Older adults in rural regions are more vulnerable to sarcopenia than those living in urban areas.19) Malatya, the province in which this study was conducted, is located in Eastern Anatolia, Turkey. People aged ≥65 years constitute 10%–12% of the total population in this province.2) This study aimed to determine the nutritional status and the risk of sarcopenia in hospitalized older adults in Malatya, a rural region in Turkey.
MATERIALS AND METHODS
The inclusion criteria of the study were individuals aged ≥65 years hospitalized at the Malatya Turgut Ozal University Medical Faculty Hospital and who volunteered to participate in the study. The exclusion criteria were people aged <65 years; those with dementia or Alzheimer disease, cognitive or mental impairment, end-stage kidney disease, or cancer, unable to communicate, or who did not agree to participate.
Data Gathering Instruments
Information collection forms were completed by researchers during in-person interviews with the patients. The questionnaire consisted of four sections containing sociodemographic data, health information, nutrition screening tests, and anthropometric measurements, respectively.
Anthropometric Measurements and Hand Grip Strength
Calf circumference
Calf circumference was measured from the widest part of the calf in the sitting position using a non-stretchable tape measure with the ankle and knee at 90°. The same measurement was performed on bedridden participants. Calf circumference reflects a change in the lean muscle mass with age.20)
Height
The presence of diseases (e.g., arthritis, osteoporosis, spinal deformity, and various neuromuscular diseases), dependence on a bed or wheelchair, and kyphotic posture that occur with aging make it difficult to accurately measure the height of older adults. Inaccurate measurement leads to misleading estimations of nutritional status. Therefore, knee length measurement is recommended to avoid this problem. The present study used the following formula to calculate height using the knee length, age, and sex.
Knee length was used to measure the correct height in elderly individuals who were bed- or chair-bound and cannot stand upright. Knee length was measured using a sliding caliper with the knee and ankle upright at 90°.
Men: 64.19 – (0.04 × age) + (2.02 × knee length)
Women: 84.88 – (0.24 × age) + (1.83 × knee length)
Body weight
The body weight of older adults who could move independently was measured with a weighing device sensitive to 0.1 kg. The participants stood on a flat, hard, and stable surface, and wore thin clothes and no shoes. During the measurements, care was taken that the participants did not lean on anything or apply any outside force.
Body mass index
Body mass index (BMI) is a practical method for detecting obesity and protein–energy malnutrition. It is calculated by dividing the body weight (kg) by the square of the height (m2). Changes in BMI in older adults vary depending on the loss of lean tissue, in addition to adipose tissue. The absence of a consensus cutoff point for the assessment of BMI in older adults reduces its validity in determining nutritional status. We applied the World Health Organization (WHO) BMI values for adults.
Hand Grip (muscle) strength
Hand grip strength was measured using a mechanical dynamometer (EASYCARE Hand Dynamometer; Fabrication Enterprises, Elmsford, NY, USA) with a scale of 0–100 kg and a precision of 1.0 kg.21) The participants were instructed to put all their strength into grasping the instrument while it was held vertically in front of them, with their free arm hanging freely from their side. The measurement was performed twice on each hand (right and left) and all three values, in addition to the mean value provided by the instrument, were recorded. These measured values were compared with reference values determined based on the participants’ age and sex.22)
GNRI
We calculated GNRI using the formula “1.489 × serum albumin (g/L) + 41.7 * (body weight in kilograms/ideal body weight).” The formula “22 × square of height in meters” was used to determine the ideal body weight. In GNRI, scores >112.3, 103.8–112.3, and <103.8 indicate mild, moderate, and severe malnutrition, respectively.23)
PNI
We calculated PNI using the formula “10 × serum albumin (g/dL) + 0.005 × total lymphocyte count (mm3).” In PNI, scores >56.1, 50.0–56.1, and >50.0 indicate normal, mild to moderate, and severe malnutrition, respectively.24)
MNA
MNA offers an easy and rapid method to evaluate the nutritional status of older adult patients in outpatient clinics, hospitals, and nursing homes. In the MNA screening test, the best option is marked. At the end of the test, the scores are summed. The screening test consists of two stages; the screening phase, followed by the evaluation phase. In the screening stage, a score of 12–14 points denotes a normal nutritional status, 8–11 points denotes a risk of malnutrition, and 0–7 points denotes malnourishment in older adults. Scores of 24–30, 17–23.5, and <17 points in the screening and evaluation sections denote normal nutritional status, risk of malnutrition, and malnutrition, respectively.25)
Evaluation of Sarcopenia Status
The evaluation of an individual's muscle mass, muscle strength, and physical performance are all necessary steps in the diagnosis of sarcopenia. Various approaches are used to assess these three aspects. We measured the total muscle mass of each participant using Lee's equation, with muscle masses <7.0 kg in men and <5.4 kg in women defined as “low.”26) We measured muscle strength using the hand strength tightening method, with grip strengths of <20.0 kg in women and <30.0 kg in men categorized as "weak" based on the older adult diagnostic algorithm from the EWGSOP. We assessed each participant’s level of physical performance using the get-up-and-go test, with <0.8 m/s as the threshold. Low walking speed was defined with <0.8 m/s as the threshold.27)
Muscle mass (kg) = (0.244 × BMI) + (7.8 × height [m]) + (6.6 × sex [M:1; F:0]) – (0.098 × age) + (ethnicity – 3.3)
where calculation of ethnicity was made by assigning values of 0, 1.4, and 1.2 for White and Hispanic, African, and Asian, respectively.
Statistical Analysis
We performed the statistical analyses using IBM SPSS Statistics for Windows (version 22.0; IBM Corp., Armonk, NY, USA). Normality was assessed visually (histograms and probability plots) and analytically (Kolmogorov–Smirnov/Shapiro–Wilk tests). The chi-square test was used to compare proportions between groups. We applied Student t-test to compare the results between groups for normally distributed continuous variables. Continuous variables are presented as means and standard deviation, whereas categorical variables are shown as percentages and numbers. We applied the Mann–Whitney U test to compare nonnormally distributed continuous parameters between the groups.
We examined the relationship between muscle mass and strength using univariate regression analysis. Odds ratios were modified for other variables including BMI, age at baseline, polypharmacy, nutritional status indicators, and malnutrition status. The univariate regression model had statistically significant variables added as potential confounders. Statistical significance was set at p<0.05.
Ethics Statement
This study was approved by the Ethics Committee of Mardin Artuklu University (Approval No. 2023/15-15). Before beginning the survey, all the respondents read a written consent form and voluntarily consented to participate.
Also, this study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.28)
RESULTS
The mean age of the study participant was 76.21±5.59 years, with 55.65% of the participants 65–74 years of age and 42.90% women. Three or more chronic diseases were present in 36.23% of the participants, and 23.48% used three or more drugs per day (Table 1). According to the sarcopenia criteria, 45.50% of the participants had sarcopenia.

General characteristics of individuals (n=345)
The results of the comparisons of age and anthropometric characteristics of the participants according to their sarcopenia status are shown in Table 2. The muscle mass, muscle strength, and calf circumference differed significantly according to sarcopenia status, with lower values in participants of both sexes with sarcopenia (p<0.05).

Age and anthropometric characteristics of individuals according to their sarcopenia status
Table 3 shows the relationships between sarcopenia and malnutrition indices of individuals according to sex. The MNA-SF and GNRI scores of participants with sarcopenia were lower than those in individuals without it for both sexes (p<0.05). The PNI scores were lower in those with sarcopenia individuals than in those without sarcopenia group in women (p<0.05) but not in men (p>0.05).
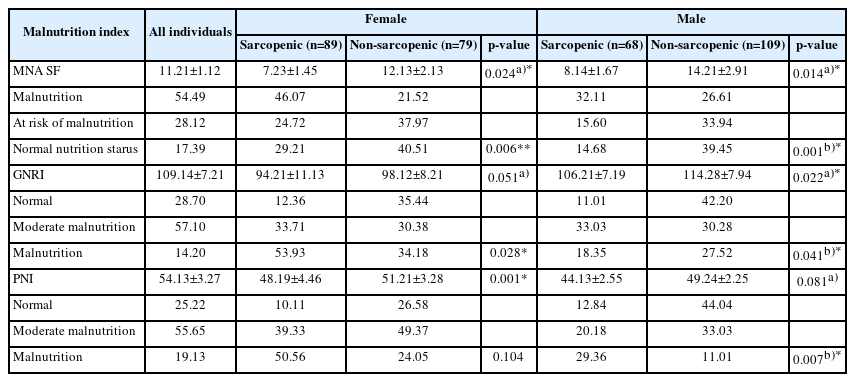
Malnutrition indices and distributions of individuals according to sarcopenia and sex
The factors affecting muscle mass and strength are listed in Table 4. The most important factor was MNA score (p<0.05), followed by age, BMI, and GNRI (all p<0.05). Muscle mass was also affected by PNI score and calf circumference (p<0.05). Muscle mass and strength in men were influenced by BMI, PNI, and GNRI scores (p<0.05). In addition, the number of prescribed drugs was an important factor affecting muscle mass in men (p<0.05) but not in women (p>0.05).

Multiple linear regression analysis of factors affecting muscle strength and muscle mass in individuals by sex
DISCUSSION
Care for older adults is a new and developing service model in Turkey. This study is one of the few that examine the nutritional status of older care patients with sarcopenia in Turkey. Our results showed that the prevalence of malnutrition is quite high in general and reflects sarcopenia in patients receiving hospital care.
In this study, 55.7% of the older adults were aged 65–74 years. According to the Turkish Statistical Institute (TSI) in 2022, 64.5% of the elderly population in Turkey is 65–74 years of age, and this age range is consistent with the proportions of hospitalized older adults.2) In the present study, 42.9% of the participants were women and 57.1% were men. According to the TSI-2022 data, the prevalence of older adult women is higher than that of men in Turkey (F, 55.7%; M, 44.3%).2) Moreover, 61.1% of women and 49% of men had visited a health institution in the last 3 months.29) One explanation for the predominance of men in this study was a higher number of hospital admissions due to the number of chronic diseases and multiple drug use rates compared to women. Sarcopenia and malnutrition are associated with negative health outcomes including falls, fractures, physical disability, frailty, poor quality of life, and mortality. Therefore, early diagnosis is important, especially in older adults, to prevent sarcopenia and malnutrition in a timely manner and allow early treatment interventions.30) BMI values of 23–29.9 kg/m2 have been associated with optimal life expectancy in older adults. The risk of death increases in older adults with BMI <23 kg/m2.31) The mean BMI values were 22.1 kg/m2 and 21.3 kg/m2 among the participants in this study with and without sarcopenia, respectively. BMI was a risk factor in both groups. Yanishi et al.32) Chien et al.33) and Siegert et al.34) reported higher BMI in individuals without sarcopenia compared to those with it. However, Prior et al.35) observed no significant differences between the BMIs of 76 middle-aged and older adults with and without sarcopenia. We observed similar results regarding BMI values as those in the study by Prior et al.35)
Regardless of BMI, malnutrition in older adults exacerbates the age-related loss of muscle mass and plays a role in sarcopenia.7) A previous study found that participants with both sarcopenia and a high risk of malnutrition have a four-fold higher mortality risk compared to participants with normal nutrition and without sarcopenia17); therefore, sarcopenia screening in conjunction with nutritional assessment is crucial.36) The components of sarcopenia are based on the loss of muscle mass and strength with poor nutritional parameters. A recent systematic review reported a sarcopenic ratio of 10% in older adults; however, the measurement instruments vary among studies.37) In this study, three different instruments used to measure sarcopenia. A hand-grip dynamometer was used to measure hand-grip strength, usual gait speed was used to gauge physical performance, and calf circumference was used as a proxy for muscle mass. The hand-grip strength thresholds recommended by the EWGSOP are <16 kg for women and <27 kg for men. EWGSOP-2 suggests that each community should set its own threshold values.14) Accordingly, the threshold values for hand grip strength in Turkey are <22 kg for women and <32 kg for men.38) In the present study, the average hand-grip strength of the sarcopenic individuals was 28.3 kg. In their study of participants with sarcopenia, presarcopenia, and no sarcopenia, Chien et al.33) reported that hand-grip strength did not differ significantly between individuals. However, the grip strength of individuals without sarcopenia was higher than that of individuals with it in the studies by Moreira et al.39) in middle-aged women in Northeast Brazil, Siegert et al.,34) Yanishi et al.,32) and Di Monaco et al.40) in 138 women, and Woo et al.41) in Chinese women and men. Similarly, in our study, the grip strength of participants with sarcopenia was lower because of decreased muscle strength. Therefore, regular follow-up of individuals with sarcopenia is important.
WHO regards calf circumference as the most accurate anthropometric standard for determining muscle mass in older adults.42) In 2019, the EWGSOP revised its criteria to include calf circumference as a diagnostic proxy for older adults in areas lacking access to other methods of diagnosing muscle mass.43) In the present study, the mean calf circumference in individuals with sarcopenia was 30.3 cm. Low calf circumference is an important predictor of mortality and frailty in older adults.44) Kusaka et al.45) reported greater right and left calf circumferences in individuals without sarcopenia compared to those with it. Similarly, we observed greater calf circumference measurements in both men and women without sarcopenia. In addition, calf circumference measurement was significantly associated with muscle mass and muscle strength in the present study.
Decreased muscle mass is a common characteristic of malnutrition and sarcopenia. Malnutrition directly contributes to the sarcopenia development. A previous study showed that the risk of developing sarcopenia was 13 times higher in malnourished or older adults at risk of malnutrition than in individuals with a normal nutritional status.46) In another study, >80% of participants with sarcopenia were malnourished or at risk of malnutrition according to the MNA.47) In the present study, the malnutrition index scores were lower in individuals with sarcopenia compared with those without sarcopenia. The most important factor affecting muscle mass and strength in both sexes was the MNA score, followed by age, BMI, and GNRI. In addition, the number of prescribed drugs was an important factor affecting muscle mass in men. Nutritional screening tools have revealed that factors affecting food intake and malnutrition are associated with sarcopenia in older adults living in rural areas. Our findings are supported by those of other studies reporting the association of sarcopenia with advancing age, low BMI, and malnutrition indices.48-50)
The most important limitation of this study was its cross-sectional design, which prevented the generalization of these findings to other older adult populations. Moreover, we were unable to use techniques regarded as gold standards to assess muscle mass, such as DEXA, computed tomography, and MRI. Instead, we substituted the calf circumference measurements for actual muscle mass. While the lack of use of these gold-standard techniques can be seen as a limitation, a strength of this study was that we optimized our measurements according to our study objectives.
In conclusion, malnutrition and sarcopenia, which are common conditions in older adults, have negative effects such as higher morbidity and mortality, as well as higher healthcare costs and rehospitalizations. A healthy diet and regular exercise can prevent these two conditions. Each condition is typically screened separately, and they are rarely assessed simultaneously. A patient's nutritional and functional status should always be assessed to discuss therapeutic interventions and lifestyle changes, as many patients exhibit both malnutrition and sarcopenia (i.e., an increase in protein intake and physical activity). The results of our study will inform future studies, since the study region is rural and has a high ratio of older adult population to the total population.
Notes
We thank all the participants. We also express our sincere thanks to Dr. Bülent Yaprak and Professor Murat Aladağ, who helped us reach the patients and reviewed the draft.
CONFLICT OF INTEREST
The researchers claim no conflicts of interest.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization, NA, HA, YS; Data curation, NA, HA, YS; Supervision, NA, HA, YS. Investigation, NA, HA, YS; Writing-original draft, NA, HA, YS; Writing-review & editing, NA, HA, YS.