INTRODUCTION
Recently, the term "osteosarcopenia" has been proposed to describe the coexistence of osteopenia/osteoporosis and sarcopenia.1) The negative effects of osteoporosis (bone loss) and sarcopenia (loss of muscle mass and function), such as increased risks of falls, fractures, frailty, disability, and early mortality, highlight the need to maintain musculoskeletal health in old age.2) Osteosarcopenia occurrence becomes more common with aging, reaching a frequency of 33.7% in individuals over 80 years of age. Mortality is also considerably higher in patients with osteosarcopenia (15.9%) than in those without (6.1%). Additionally, individuals with osteosarcopenia have a higher incidence of fractures, falls, and functional impairment compared to those without osteosarcopeniaŌĆöfall: hazard ratio (HR)=1.60; 95% confidence interval (CI), 1.07ŌĆō2.38; p<0.05; fractures: HR=1.54; 95% CI, 1.13ŌĆō2.08; p<0.01; functional impairment: HR=1.83; 95% CI, 1.41ŌĆō2.38; p<0.001.3)
Osteoporosis is one of the most prevalent public health problems and a significant risk factor for adverse health outcomes, including fractures.4) Sarcopenia, an age-related decline in skeletal muscle mass, strength, and function, is defined by the degeneration of muscle quantity and quality, frequently resulting in severe unfavorable effects.5) Increased attention has been paid to osteoporosis and sarcopenia, as the two conditions together have been called a ŌĆ£hazardous duetŌĆØ that worsens health consequences.4-6) The concept of a bone-muscle unit suggests communication between these tissues; hence, diseases that affect one element of the musculoskeletal unit are likely to impact the other, and vice versa.7) However, to date, there is a dearth of evidence from randomized controlled trials (RCTs) that have studied a shared pharmacological target for osteosarcopenia even though therapeutic targets common to both bone and muscle have been postulated.7)
The current recommendations for the treatment of osteosarcopenia include non-pharmacological and pharmacological treatments. Diet and exercise are the cornerstones of non-pharmaceutical treatments. The Framingham Osteoporosis Study reported that low protein consumption was related to bone loss in the proximal femur and spine during a 4-year period.8) Protein consumption is beneficial for enhancing muscle mass,9) while the effects on sarcopenia-related measures, such as strength and functional capacity, are less consistent,9,10) and the effects of exercise are enormous.11) As a non-pharmacological treatment for osteosarcopenia, these two treatments should be combined. Numerous Food and Drug Administration (FDA)-approved drugs are widely available,12) however, no approved pharmacological medicines exist for the treatment of osteosarcopenia. Testosterone, denosumab, growth hormone, and anti-myostatin antibodies have all been studied as potential pharmacological treatments for osteosarcopenia, although the results have been inconsistent. Denosumab, a human monoclonal antibody, has shown encouraging results in the treatment of osteosarcopenia.13) In bone, denosumab binds to the cytokine RANKL with high specificity and affinity to limit its effect. Consequently, osteoclast recruitment, maturation, and action are blocked, and bone resorption slows.14) Denosumab may also affect muscle mass through the inhibition of the receptor activator of nuclear factor-B ligand (RANK/RANKL) by enhancing muscular strength and balance in older individuals at risk for falls and fractures.15)
Several studies and meta-analyses have been conducted to assess the role of nutritional intervention and exercise in osteosarcopenia; however, the treatment of osteosarcopenia with pharmacological drugs is a novel area of exploration, and evidence on this topic is scarce. Nonetheless, the therapeutic effects of some substances on osteoporosis and sarcopenia suggest a potential dual effect on muscle and bone mass, which may be effective in treating osteosarcopenia.7) We conducted a comprehensive review and meta-analysis to analyze the present data and provide evidence regarding the therapeutic efficacy of denosumab and assess whether denosumab can be the treatment of choice for patients with osteosarcopenia compared to bisphosphonate, which is currently the gold standard for treating osteoporosis.
MATERIALS AND METHODS
Eligibility Criteria
We included all research articles that analyzed the therapeutic effects of denosumab for the treatment of osteosarcopenia. We independently screened the eligible publications were screened using the following inclusion criteria: (1) patients with osteosarcopenia or osteoporosis, (2) English language, and (3) original articles. We excluded non-research articles (e.g., case reports or series, review articles, letters to the editor, study protocols, editorials, or commentaries) and studies with insufficient data. The PICO (Population, Intervention, Comparator and Outcomes) framework was used to set the eligibility requirements (Table 1).
Search Strategy and Study Selection
This meta-analysis was performed according to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow statement. We systematically searched the PubMed and the Cochrane Central Register of Controlled Trials (CENTRAL) databases using the following search terms: (ŌĆ£osteoporosisŌĆØ AND ŌĆ£sarcopeniaŌĆØ) AND (ŌĆ£denosumabŌĆØ OR ŌĆ£antibodies, monoclonal humanizedŌĆØ) with the latest search performed on October 19, 2022. Articles were independently screened for relevance based on their abstracts. These articles were thoroughly read and those that fulfilled our criteria were included in the study. The final inclusion of the studies was based on the agreement of all authors. Any disagreement was settled by author consensus, in which the agreement of more than two authors was the final decision. The full texts of the remaining articles were assessed according to the inclusion and exclusion criteria. The quality of the studies was assessed using a checklist guide from the Joanna Briggs Institute (JBI) critical appraisal tool based on study design. We used a cutoff point to determine the quality of the studies. We used a cutoff point of half of the total score on each JBI critical appraisal checklist. Low-quality studies had scores below the cutoff point, while the rest were considered high-quality studies.
Data Extraction
Data extraction was performed independently by all authors using standardized forms that included author, year of study, study design, country of study, number of subjects, location of study, subject ages, T-score in the lumbar spine (LS), study duration, subject handgrip strength, subject gait speed, study description of, and comparator drugs. The main outcome of the studies was the mean difference (MD) between change in bone mineral density (BMD) in the LS, change in handgrip strength, and change in gait speed. The changes in BMD in the LS, handgrip strength, and gait speed were defined as the differences between baseline and after denosumab treatment during the observation period. BMD was calculated using a dual X-ray absorptiometry (DXA) scan and expressed in g/cm2, handgrip strength was expressed in kg, and gait speed was expressed in m/s within 4 minutes of walking.
Definition of Osteosarcopenia
Osteoporosis was radiographically diagnosed based on BMD measurements as a DXA T-score of Ōēż-2.5.16) The diagnostic criteria for sarcopenia were based on the Asian Working Group for Sarcopenia (AWGS) criteria, which define sarcopenia as low handgrip strength (<26 kg for men and <18 kg for women) and/or low gait speed (Ōēż0.8 m/s both for men and women) and low muscle mass (<7.0 kg/m2 for men and <5.7 kg/m2 for women).17) Sarcopenia was confirmed by the presence of low muscle quantity or quality. The presence of low muscle strength, low muscle quantity/quality, and low physical performance was considered severe sarcopenia.18) No further criteria exist for defining osteosarcopenia beyond the combination of the clinical and imaging criteria for low BMD and sarcopenia described above. In other words, osteosarcopenia is the presence of sarcopenia with osteopenia or osteoporosis.19)
Statistical Analysis
RevMan v5.4.1 (Copenhagen, Nordic Cochrane Center; The Cochrane Collaboration, 2020) was used to perform the meta-analysis by computing the MD and 95% confidence interval (CI) for the osteosarcopenia parameter (changes in BMD in LS, handgrip strength, and gait speed) from baseline to the study endpoint for the placebo or other agent treatments and denosumab treatments. The p-value was two-tailed, and statistical significance was set at p<0.05. Heterogeneity was assessed using the Q-statistic and I2 test. The I2 statistic measures the percentage of total variation across the studies due to clinical or methodological heterogeneity rather than chance. A random-effects model was used in the analysis to better represent the population. Publication bias was assessed by visual inspection of funnel plots.
RESULTS
Baseline Characteristics and Study Selection
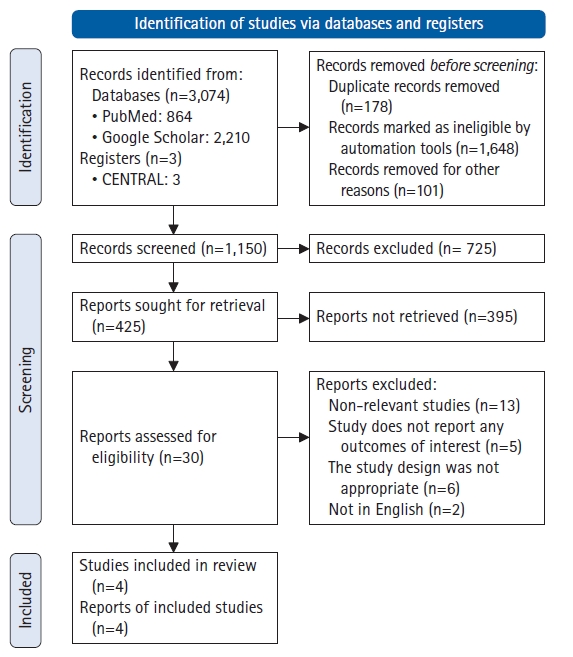
The initial search strategy identified 3,074 studies. Following this, 3,044 papers were excluded based on title and abstract screening, as well as other factors, leaving four relevant studies. Studies that lacked the necessary data for this meta-analysis, or those that were retracted, were excluded. After screening and qualitative analyses, we included four papers in our study. Fig. 1 presents the PRISMA 2020 flowchart.
The meta-analysis included two RCTs and two cohort studies. Between 2019 and 2022, 264 and 244 samples in the intervention and control groups, respectively, appeared in these publications. Denosumab was administered to the experimental group for 6 months to 5 years, whereas the control group received oral alendronate 70 mg once weekly, 5 mg intravenous zoledronate once yearly, or 3 mg ibandronate intravenously every 3 months. Table 2 provides an overview of the findings and the investigational characteristics.20-23) We examined the risks of bias for cohort and RCT trials using the JBI critical appraisal tool. Each of the four articles passed the quality evaluation. The results of the risk of bias analysis are detailed in Supplementary Tables S1ŌĆōS5.
Denosumab Administration for Osteosarcopenia
Effect of denosumab on LS BMD change
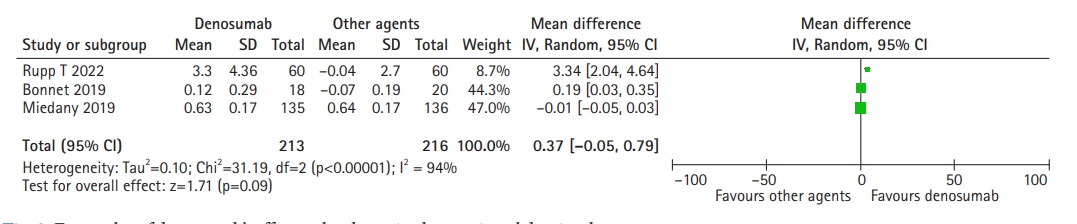
Compared to other agents, such as zoledronic acid, ibandronate, or alendronate, no significant differences were observed in LS BMD change when denosumab was administered. Based on the random-effects model (I2=94%; Žć2=31.19; p<0.00001), the pooled mean difference between denosumab and other agents was 0.37 g/cm2 (95 CI, -0.05ŌĆō0.79; p=0.09) and did not differ significantly regarding LS BMD change (Fig. 2).
Effect of denosumab on handgrip strength change
Our meta-analysis showed that denosumab had a significant effect on handgrip strength change compared to standard agents such as zoledronic acid, ibandronate, and alendronate. Based on the random-effects model (I2=60%; Žć2=5.03; p=0.08), the pooled mean difference between denosumab and other agents was 5.16 (95% CI, 1.38ŌĆō18.94; p=0.007) and showed a significant improvement in handgrip strength (Fig. 3).
Effect of denosumab on gait speed change
The 4-m walk gait speed was used to evaluate the effect of denosumab on gait speed compared to other agents. Denosumab had no significant effect on gait speed change compared to standard agents such as zoledronic acid, ibandronate, and alendronate. Based on the random-effects model (I2=100%; Žć2=597.58; p<0.00001), the pooled mean difference between denosumab and other agents was 0.11 (95% CI, -0.18ŌĆō0.40; p=0.46) and showed no significant differences in gait speed change (Fig. 4).
Effect of denosumab on ALM
The ALM was significantly higher in the denosumab group than that in the bisphosphonate group. After 3 years of denosumab administration, ALM increased in the bisphosphonate group (3.22┬▒10.0 kg vs. -0.07┬▒6.6 kg). Changes in ALM were strongly correlated with changes in LS BMD (r2=0.82; p<0.001) in the denosumab group but not in the other groups.20) Women with osteoporosis receiving anti-osteoporosis agents in the treatment group, such as bisphosphonate alone in 60 patients, bisphosphonate with activated vitamin D3 in 12 patients, selective estrogen receptor modulator in four patients, and others in six patients, showed no difference in ALM change compared to placebo after 10 years. The baseline ALM before treatment in the bisphosphonate group was 14.1┬▒1.4 kg versus 14.1┬▒1.7 kg in the placebo group. After 10 years of follow-up, the ALM values were 13.9┬▒1.5 kg versus 13.9┬▒1.7 kg in the treatment group versus the control group. The change in ALM did not differ significantly between the bisphosphonate and control groups (-0.2┬▒0.9 kg vs. -0.2┬▒0.9 kg; p=0.543).24) The funnel plots of all analyses in our study did not reveal any significant asymmetry.
Effect of denosumab on FN BMD change
Rupp et al.22) showed that denosumab also has better outcomes in FN BMD compared to bisphosphonate. The mean annual percentage changes in FN BMD were higher in the denosumab and bisphosphonate groups and were significantly higher compared to the basic groupŌĆömean FN BMD in % change per year: basic (-0.78%┬▒2.12%), bisphosphonate (0.68%┬▒2.54%), and denosumab (1.83%┬▒2.66%). We also present some results on the effect of denosumab on ALM and FN BMD changes as secondary outcomes; however, we did not perform statistical analysis due to the limited number of studies and lack of data.
DISCUSSION
Osteosarcopenia is a common but potentially preventable and treatable illness; if not addressed promptly, it can result in falls, fractures, loss of self-sufficiency in everyday activities, and mortality.25) A study of 680 older adult patients with osteosarcopenia in Sydney reported an increased incidence of falls and fractures.26) Osteosarcopenia is a potentially preventable and treatable disease. Most therapeutic therapies address low BMD and sarcopenia individually; however, the close relationship between the two disorders implies that an integrated interventional approach is more likely to be effective.27) Several drugs are already used to prevent fractures caused by osteoporosis.
The current treatments for osteoporosis fall into two categories: anti-resorptive (bisphosphonates and denosumab) and anabolic (teriparatide and abaloparatide). Anti-sclerostin antibody is another innovative osteoporosis medication with an anabolic effect that remains under investigation.26) Currently, anti-resorptive agents are more widely used than anabolic agents for the treatment of osteoporosis. Although pharmacological interventions for osteoporosis have been extensively explored, data and evidence for pharmacological interventions for osteosarcopenia are currently inadequate. Denosumab is a human immunoglobulin G2 monoclonal antibody with excellent affinity and specificity for RANKL.28) RANK, its ligand RANKL, and the soluble decoy receptor osteoprotegerin (OPG) pathway are primarily responsible for bone remodeling and homeostasis. The binding of RANKL to its associated receptor RANK initiates a series of signaling events that cause osteoclast development, activity, and survival.21) Several studies have demonstrated a strong link between osteoporosis and skeletal muscle dysfunction; however, the molecular mechanism regulating bone and skeletal muscle pathology remains unknown.21)
The results of our meta-analysis demonstrated the lack of significant differences in the effect of denosumab on LS BMD change compared to other agents like zoledronic acid, ibandronate, or alendronate, with a pooled mean difference between denosumab and other agents of 0.37 g/cm2 (95% CI, -0.05ŌĆō0.79; p=0.09). In head-to-head tests comparing denosumab and bisphosphonate, the denosumab group exhibited comparable BMD changes at all four bone locations compared to the alendronate group. Alendronate and denosumab at the LS were also associated with significant increases in BMD (p<0.001) compared to placebo.29) However, a meta-analysis of 11 studies that included head-to-head comparisons of 2,573 participants taking bisphosphonates and 2,873 participants taking denosumab reported results contrary to those in our meta-analysis, which suggested that denosumab significantly increased BMD at the hip, femoral neck, LS, and one-third radius but did not significantly reduce fracture risk.30) The most likely reasons for this outcome difference compared to our study are the superior adherence, compliance, and denosumab durability compared to bisphosphonate. The mode of administration for denosumab requires subcutaneous injection by healthcare providers, which provides direct proof of patient adherence to therapy.31) This may also be attributed to the mechanisms of action of each medicine. Denosumab, a new anti-resorptive drug, suppresses osteoclast-mediated bone resorption similarly to bisphosphonates, but via a different mechanism.32) The actions of bisphosphonates in preventing bone loss rely mostly on bisphosphonate binding to bone minerals, while denosumab inhibits osteoclast survival and differentiation mostly by direct interaction with RANKL.30) Oral bisphosphonates and subcutaneous injectable denosumab are currently the recommended agents for the treatment of osteoporosis; of these two drugs, oral bisphosphonates are considered the first-line therapy.33) In terms of the reduction of osteoporosis fracture risk, neither medication differed significantly from the others. Pedersen et al.34) performed a retrospective cohort analysis of the risk of hip fractures in individuals treated with denosumab and alendronate, reporting comparable hip fracture risk ratios for denosumab and alendronate independent of sex, age, or fracture history.
As described above, osteosarcopenia is a term used to describe older persons with both poor BMD and sarcopenia. Sarcopenia is defined as the presence of decreased muscle mass accompanied by diminished muscular function, strength, and performance.5) We performed a meta-analysis to determine whether denosumab has a distinctly favorable influence on sarcopenia parameters. We used measurements of the changes in handgrip strength following denosumab injection to evaluate muscle strength. After denosumab treatment, we measured physical performance by quantifying the change in gait speed, while ALM was used to determine muscle mass. Because of its simplicity, uniformity, and strong connection with lower-extremity muscular strength, handgrip strength is the most preferred method to test muscle strength.18) In addition, handgrip strength is a clinical indicator of limited movement and a predictor of clinical outcomes.5) The results of our meta-analysis showed that denosumab significantly improved handgrip strength compared to other agents including zoledronic acid, ibandronate, and alendronate. Based on the random-effects model, the pooled mean difference between denosumab and the other agents was 5.16 kg (95% CI, 1.38ŌĆō18.94; p=0.007). In an observational prospective study, Pizzonia et al.35) reported that denosumab increased handgrip strength. Handgrip longitudinal (T0ŌĆōT1) measurements were reported in 31 female patients. A T0ŌĆōT1 MD was reported in 19/22 patients treated with alendronate (0.85┬▒4.8 kg) and in 12/13 females treated with denosumab (0.97┬▒6.0 kg), respectively, indicating a positive handgrip trend over time. However, the authors did not investigate the significance of these differences in either group.
The results of our meta-analysis showed that denosumab had no significant effect on gait speed change compared to placebo or other agents, such as zoledronic acid, ibandronate, or alendronate. Based on the random-effects model, the pooled MD between denosumab and other agents was 0.11 (95% CI, -0.18ŌĆō0.40; p=0.46) and showed no significant differences in gait speed change. To date, little research has reported the effects of denosumab on gait speed. Miedany et al.21) reported that denosumab not only enhanced BMD but also decreased the risk of falling. Compared to bisphosphonates, denosumab exhibited the most substantial favorable effect on physical performance, as indicated by the improvement in the 4-m walk test (p<0.001 in the denosumab group vs. p=0.05 in the alendronate and zoledronic group) to measure gait speed.21) These contradictory findings may be a consequence of the numerous variables that impact gait speed. Gait speed diminishes with age, is controlled by various variables, and can be improved by adopting a lifestyle that strengthens the muscles of the lower extremities.36) However, a study by Miedany et al.21) did not specifically identify confounding variables that might influence gait speed in their study population. Denosumab-induced increases in BMD did not necessarily correlate with increased gait speed. In older adult men, agility and gait speed showed the greatest influence on BMD and structure, whereas balance was associated with BMD in older adult women.37) One study found that older adult women with more rapid bone loss during 2 years of follow-up had a greater risk of decline in usual walking speed compared to those with higher BMD.38)
Although our meta-analysis did not directly examine ALM changes due to restricted research data, denosumab treatment may also help improve ALM in older individuals with osteoporosis. ALM levels significantly increased in the denosumab group compared to those in the bisphosphonate group after 3 years of administration.20) The binding of denosumab to RANKL and its associated receptor RANK results in a cascade of signaling events that induce osteoclast development, activity, and survival. OPG is a soluble decoy receptor that binds to RANKL, thereby inhibiting its interaction with RANK and reducing osteoclastogenesis and bone loss.39,40) Recent studies have highlighted the significance of mutual communication between muscle and bone via myokine and osteokine release, indicating that the treatment of osteoporosis with anti-osteoporotic drugs may also have a positive effect on muscle condition.24)
The RANK/RANKL/OPG pathway is important for more than just bone health and may play a role in skeletal muscle and other tissues.41) A mouse investigation showed high RANKL expression in the bone and muscle, notably in the soleus, compared to other muscles (gastrocnemius) and soft tissues, such as the colon, liver, and white and brown adipose tissues. RANK has also been detected in muscle, but to a lesser extent than in bone20) and skeletal muscles. As a result of NF-╬║B activation, RANKL/RANK signaling in skeletal muscle inhibits myogenic development, leading to skeletal muscle dysfunction and atrophy.42) In a mouse model of Duchenne muscular dystrophy and denervation-induced muscle atrophy, the injection of recombinant OPG protein resulted in enhanced muscle strength. More recently, the effects of inhibiting RANKL and RANK on muscle mass and strength have also been reported in conditions such as osteoporosis and sarcopenia.20) Mice containing the human RANKL genomic region (huRANKL-Tg mice) had lower muscle mass, force, fat infiltration, and glucose absorption as well as a low bone mass phenotype and increased expression of anti-myogenic and inflammatory genes.
Denosumab is a monoclonal antibody that targets RANKL.28) Bonnet et al.20) studied insulin signaling in C2C12-differentiated myotubes expressing both RANK and RANKL to better understand the effect of RANKL-RANK signaling on muscle cell metabolism. In these cells, RANKL enhanced Ser318 phosphorylation in insulin receptor substrate-1 (IRS1), which is known to downregulate insulin receptor activity, whereas OPG diminished it. In contrast, AKTser473, a key IRS1 activator, showed the opposite effect.20) Consequently, the beneficial effects of OPG on insulin receptor signaling were validated in vivo in both huRANKL-Tg+ and PparbŌĆō/ŌĆō mice, as evidenced by the improved insulin tolerance test (ITT) curves.43) Through stimulation of the IkB kinase/NF-╬║B pathway, TNF-╬▒-induced inflammation in fat has been demonstrated to reduce IRS1's capacity to transduce insulin signals.44) Protein tyrosine phosphatase receptor gamma (PTP-RG), a tyrosine phosphatase receptor, has recently been identified as a crucial link between liver inflammation and insulin resistance.20) In the muscle, RANKL increased levels of PTP-RG, which were lowered by OPG-Fc in C2C12 myotubes and similarly diminished by denosumab in the soleus of huRANKL-Tg+ mice.45) Thus, RANKL causes resistance to insulin signaling, which leads to poor glucose entry, while also causing limited production of inflammatory markers (such as PTP-RG and TNF-╬▒), which may contribute to impaired glucose uptake and muscle dysfunction.44) Changes in skeletal muscle glucose uptake have been previously described,43) which reduce contractile characteristics and muscle function.20)
Treatment with recombinant OPG protein or denosumab restored muscle mass, function, and glucose consumption in huRANKL-Tg mice and peroxisome proliferator-activated receptor ╬▓ (PPAR╬▓)-deficient mice, which have a combination of sarcopenia and a low bone mass phenotype. Denosumab therapy for more than 3 years has also been observed to improve ALM and handgrip strength in osteoporotic women. While RANKL/RANK signaling reduces muscular strength, denosumab therapy may protect both bone and skeletal muscle functions.46) The results of the aforementioned studies demonstrate the potential dual effect of denosumab on BMD and muscle strength in patients with osteosarcopenia.
In conclusion, denosumab was more effective than bisphosphonate and placebo for improving muscle strength (handgrip strength). Therefore, denosumab may be favored in individuals with osteosarcopenia to improve muscular performance and reduce the risk of falls. Further research is needed to investigate the potential dual role of denosumab as an anti-resorptive and for other muscle-related impacts in this highly vulnerable population of patients with osteosarcopenia.