Factors Affecting Long-Term Care Preferences in Turkey
Article information

Abstract
Background
This study aimed to identify the long-term care preferences and the factors affecting theses preferences in Turkish society, where long-term care may soon become an important issue.
Methods
We applied data from the Family Structure Survey of Turkey conducted in 2016. Using data from 35,475 individuals, we performed descriptive analysis and logistic regressions to determine the preferences and determinants of individuals based on the Andersen Behavior Model.
Results
Informal care was the main preference of individuals living in Turkey (37%). Men, individuals living in an extended family, and the young mostly favored informal care, while women, well-educated individuals, and urban individuals preferred institutional or formal care at home.
Conclusion
Efforts should be made to raise individuals’ awareness regarding existing long-term care services. These services should be strengthened in line with society's preferences, considering regional differences.
INTRODUCTION
The demographic change due to increasing life expectancy and a decreasing fertility rate causes the aging of a society.1) Globally, the number of people aged 60 years or above is expected to double by 2050.2) Although 9.7% of the total population in Turkey is aged 65 years and over, this proportion is predicted to increase to 16.3% in 2040 and 22.6% in 2060. In other words, nearly one in four people will be over 65 years of age in 2060.3)
Despite currently lagging behind developed countries in terms of population aging, Turkey is facing an increasing number of aged people. In addition, sociodemographic changes reduce the support of informal caregivers and increase the demand for formal care. This situation underscores the need for the development of policies on long-term care (LTC) services before the situation becomes severe. Since public acceptance contributes to policy effectiveness, it is critical to identify the LTC preferences of society before implementing LTC policies.
LTC is defined as "a variety of ongoing health and social services provided for individuals who need assistance continuously because of physical or mental disability".4) While the need for LTC is not age-related, the need increases with age.1,5) These services can be categorized as home care (informal or formal), institutional care, and cash benefits. Given the cost of services, many countries build their LTC systems predominantly to strengthen home care.6-9) Individuals also prefer to receive services in their homes.10,11) However, it is not always possible to provide these services. The absence of a family member prevents informal care at home. In some cases, despite the availability of a suitable family member for informal care, avoidance of support may occur owing to the heavy burden of care.12)
Although individuals are more willing to stay in their own homes in old age, factors such as age, sex, dependency level, and the presence of chronic diseases and cognitive disorders impact the care preferences of individuals.6,12-14) Individuals' personal preferences may differ regarding receiving care at home (formal or informal) or in an institution.15-17) Several studies have reported that individuals who live alone, women, and younger people prefer institutional care.13,18) In contrast, men generally prefer informal care.13,18,19) Studies have also shown a positive relationship between individuals' education level and their preferences for institutional (or formal) care.20) Guo et al.10) reported that the LTC preference depends significantly on the severity of an individual's health impairment. Matsumoto et al.19) highlighted the effects of neighborhood environmental factors on LTC preference, in which people living in difficult areas with limited access to markets, hospitals, and transportation options preferred to relocate rather than remain in their homes when bedridden.
Today, many countries improve their LTC systems according to the socio-demographic characteristics, culture, and values of their societies.21) No uniform system can be applied to every country.22) The demand characteristics play a crucial role in the planning of LTC services. In particular, factors such as (1) individuals' preferences for institutional or home care and (2) the availability of informal support should be considered in shaping care workers and financing.
The Andersen Model, originally developed to determine the factors affecting the utility of healthcare services, is also frequently used to identify the factors affecting the preferences for LTC services.16,20,23) The many factors driving the use of services can be classified into three groups: predisposing, enabling, and need. Predisposing factors include demographic characteristics, health beliefs (attitudes, beliefs, and information on healthcare), and socio-economic status indicators. Enabling factors refer to personal and community resources that facilitate service use, including the availability of health personnel and facilities and the means and knowledge of access to them. Lastly, need factors address subjectively perceived and/or professionally assessed health status.16,17,24,25)
The present study aimed to identify LTC preferences and the factors affecting those preferences in Turkish society based on the Andersen Behavior Model.23) Understanding the preferences and the affecting factors is important for providing human-centered care, which is essential for effectively delivering high-quality LTC. As LTC will soon become an important issue in Turkey, the early identification of these preferences and the significant factors influencing them are critical for effective policymaking.
LTC in Turkey: Caregiving for Older and Dependent People
Turkey currently has no universal coverage system for LTC. Only individuals meeting the criteria regarding means-testing and dependency level can benefit from public LTC services.26) Additionally, high-income individuals can receive services from private service providers. Although services are mainly provided by public or private organizations, local governments and non-profit organizations play roles in service delivery, even if their shares are small.27,28)
The latest data show that Turkey's expenditure on LTC services is 0.22% of its GDP.29) At the same time, the general budget finances public services, while the services provided by municipalities and other public institutions are covered by their budgets. Private LTC services are based on out-of-pocket payment. LTC insurance does not exist and private health insurance policies do not cover LTC services.
These services can be roughly divided into in-kind services and cash benefits. Almost 30,000 people are residents of 451 nursing homes, of which 267 are private, 163 are public, and 21 are non-profit organizations. In addition to nursing homes, 256 public and 295 private care and rehabilitation centers also exist. In addition, Turkey has 152 public centers in the form of "Hope Houses," where two to four individuals in need of LTC live together.30)
Cash benefits for informal care are provided to strengthen informal care and help individuals and their families in need. About half a million people benefit from this assistance annually, which implies that approximately ten billion Turkish liras are distributed annually.30)
High urbanization rates, shrinkage in family structure, changes in the role of women in the family, and increased participation in working life negatively affect informal LTC.8,31) However, it remains the main source of care, as the rate of informal care provided by family members is still quite high in Turkey. Women mostly provide care to their families, such as spouses, children, and daughters-in-law.32,33) According to the Family Structure Survey, care is mostly provided by brides (28%), daughters (23%), spouses (18%), and sons (14%) in households with older adults requiring care. Only 2% of households have paid caregivers.34)
In Turkey, due to the effect of traditional family structure and culture, individuals prefer to receive care in their homes. Kurtkapan35) showed that this is true for younger individuals, as 79% reported a preference for home care. Asayesh and Ozben36) reported the reasons for preferring nursing home stays in different regions. Accordingly, the reasons for preferring nursing home stays in Western Turkey included not being a burden to the family and not being alone. In contrast, the lack of care support from their children or families (or relatives) is the predominant motivation for nursing home stays in eastern Turkey.36) In addition, Kilic and Selimen37) investigated the reasons for the preferences for nursing home stays among people aged >65 years in Istanbul, the most developed part of Turkey. In their study, 25.3% of individuals preferred to stay in the nursing home, 23% owing to the lack of care support by their children, 16.4% because of loneliness, and 6.4% due to being exposed to physical abuse.
MATERIALS AND METHODS
In this quantitative study, secondary data were analyzed. We used data from the Family Structure Survey, a nationwide cross-sectional survey conducted by the Turkish Statistical Institute (TurkStat) in Turkey in 2016. The survey collected social, demographic, economic, and health data from 35,475 individuals living in Turkey.
We performed logistic regressions by establishing binary and multinomial logit models. The binary logit model identified factors affecting the probability of selecting institutional care over home care. The estimated effects (coefficients) were the effects of log odds rather than the LTC preferences. We also calculated the marginal effects to determine the direct effects of the variables on the likelihood of choosing institutional care over home care (formal or informal).
The second model revealed the factors affecting the probability of selecting formal or institutional care over informal care at home. Because the LTC preferences were not in any particular order, a multinomial logit design was used to determine how the factors in the model affected each other.
The outcome variables in the models were generated using a specific question investigating the LTC preferences of individuals. The possible responses were formal care at an institution, informal care by a son, informal care by a daughter, and formal care at home. Thus, the first option corresponded to formal care at an institution, the next two options to informal care, and the last option to formal care at home.
We classified the factors according to the Andersen Model.23) The predisposing factors were age, sex, marital status, educational status, and living arrangement. The enabling factors were income, residential status, region, housing type, and number of children in the household. Finally, the need factors were the health status and level of happiness of the family. Table 1 summarizes the statistics of the variables used in the models.
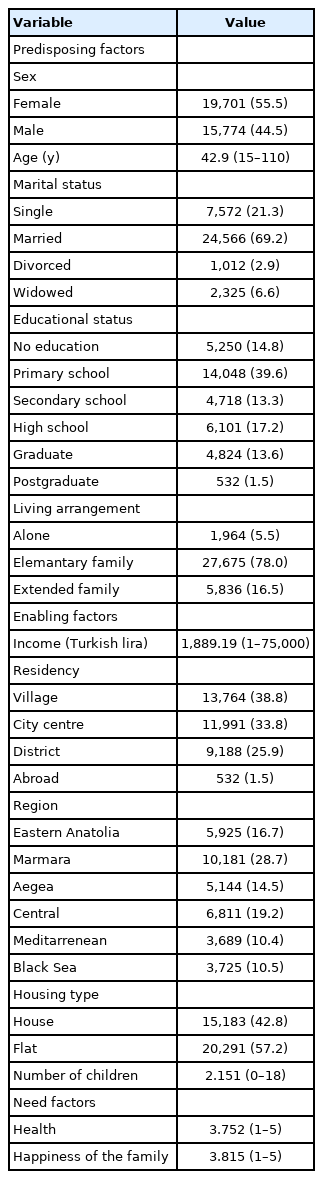
Description of the variables
Ethical approval was not required. This study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.38)
RESULTS
In this study, 12% (n=4,188) of the respondents selected institutional care, 30% (n=10,631) selected formal care at home, 37% (n=12,990) selected informal care, and 21% (n=7,666) had no preference. Individuals without an LTC preference were not included in the analyses (Fig. 1).

Distribution of the respondents across the preferences of long-term care.
Institutional Care vs. Home Care (Informal or Formal Care)
The findings are summarized in Table 2. We observed that an individual's age had a negligible effect on the probability of selecting institutional care over home care. Men were less likely to choose institutional care compared to women. Marital status showed divergent effects on LTC preference. Divorced individuals were almost 10% more likely to select institutional care compared to single individuals, whereas widowed individuals were almost 10% less likely to select institutional care. Individuals with more education were more likely to choose institutional care than people with no education.
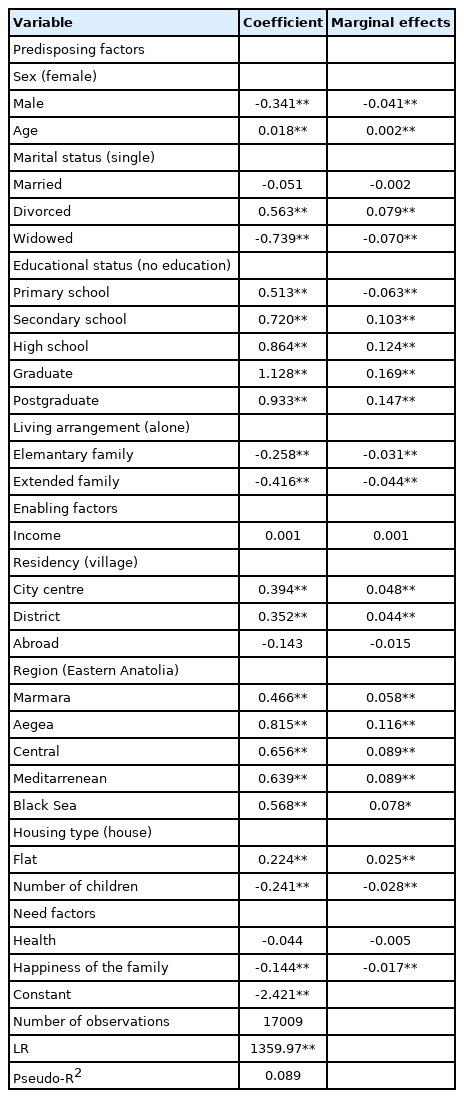
Formal care at nursing home (institutional care) vs. formal or informal care at home
Additionally, although the marginal effects are small, individuals with extended or elementary families were almost 5% less likely to select institutional care. Income was not associated with LTC preference, although we observed notable effects of residential and regional status. Individuals living in city centers and districts were almost 5% more likely to select institutional care over home care compared to their counterparts living in villages. In addition, all other regional categories were more likely to select institutional care compared to individuals living in Eastern Anatolia. Individuals living in flat areas were more likely to choose institutional care compared to individuals living in houses. An increased number of children in the house was associated with a 3% reduced chance of choosing an institution over home care.
Surprisingly, we observed no significant effects of health status on LTC preferences, whereas increased family happiness was associated with a decreased likelihood of choosing institutional care over home care.
Formal Care at Home vs. Informal Care at Home (Panel 1)
Table 3 presents the results of the multinomial logit estimation. Men were two-fold (1/0.489) less likely to select formal care at home over informal care. In addition, the logarithmic chance of selecting formal care at home increased with increasing respondent age. All marital categories placed in the model were less likely to select formal care at home compared to single individuals, which was the reference category. Compared to their single counterparts, widowed people were approximately four times less likely to choose formal care at home.
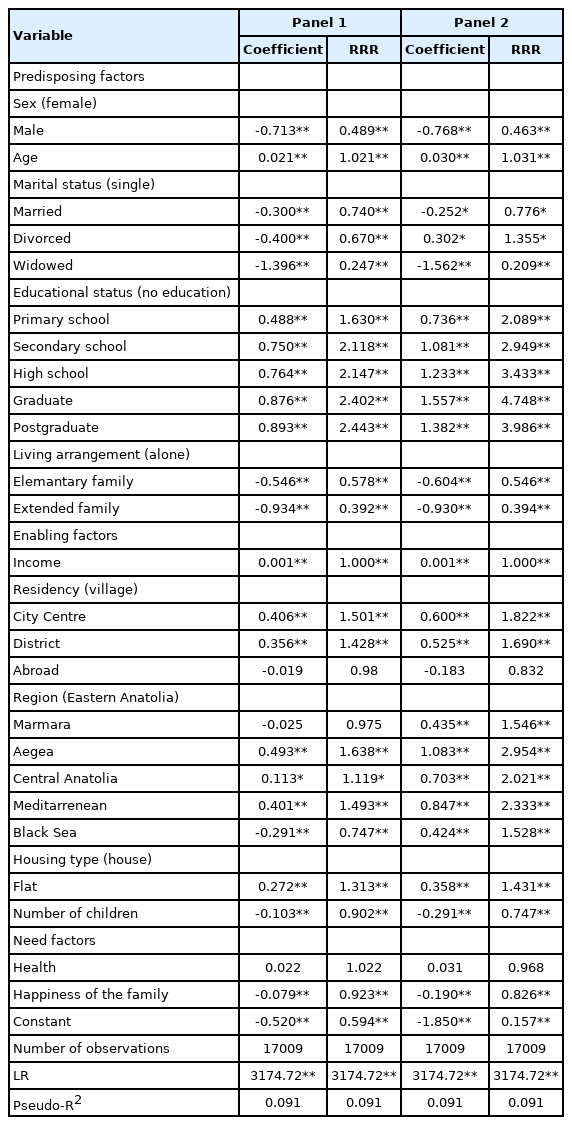
Multinomial logit model estimation results between formal care at home vs. informal care at home (Panel 1) and institutional care vs. informal care at home (Panel 2)
We observed a trend in which more educated individuals were more likely to select formal care at home over informal care. Regarding living arrangements, individuals living with their immediate or extended family were 1.73 (1/0.578) and 2.55 (1/0.392) times less likely to select formal care at home, respectively. The probability of selecting informal care tended to increase with increasing family size. However, the respondent’s income was not associated with LTC preference, although the estimated coefficient was not statistically significant. Individuals living in city centers or districts and the Aegean, Central Anatolian, and Mediterranean regions were more likely to select formal care at home over informal care compared to their village-residing counterparts.
In contrast, individuals in the Black Sea region were less likely to select formal care at home over informal care compared to individuals in Eastern Anatolia. Respondents living in flats were more likely to select formal care at home compared to respondents living in houses. Finally, a one-unit increase in the number of children in the household was associated with a decrease in the logarithmic chance of selecting formal care at home over informal care. Moreover, an individual's health status did not significantly impact their LTC preference. Finally, increased family happiness was associated with decreases in the logarithmic chance of selecting formal care at home, suggesting that happier families were more likely to select informal care.
Institutional Care vs. Informal Care at Home (Panel 2)
Compared to women, men were approximately two-fold (1/0.46) less likely to select institutional care. In addition, the logarithmic chance of selecting institutional care increased with increasing respondent age. Divorced individuals were more likely to select institutional care, while married and widowed people were less likely to select informal care compared to their single counterparts. Widowed individuals were nearly five times less likely to select institutional care (1/0.209) compared to single individuals. All educational categories were more likely to select institutional care (over informal care at home) compared to individuals with no education. In addition, we observed a trend in which more educated individuals were more likely to choose institutional care (despite the relative risk ratio of postgraduates being lower than that of university graduates). Finally, individuals living with their elementary or extended families were 1.83 or 2.53 times less likely to select institutional care, respectively, compared to their lone counterparts. Income did not affect the LTC preferences. Individuals living in city centers and districts were more likely to select institutional care over informal compared to those living in villages. In addition, all regional categories were more likely to select institutional care than their Eastern Anatolia counterparts. Individuals living in flat areas were also more likely to select institutional care compared to those living in houses. Finally, the logarithmic chance of selecting institutional care tended to decrease with an increasing number of children. Thus, an individual's health status does not affect his/her preference for LTC, whereas an increasing level of happiness in the family decreases the probability of selecting institutional care over informal care.
DISCUSSION
Using the Anderson Model, this study explored LTC preferences and their determinants in Turkey. The findings of the study confirmed the findings in the existing literature suggesting that individuals desire to live in their own homes at older ages.6,10,16,25,39) Additionally, the preferences for LTC were linked to age, sex, education level, marital status, family type, number of children in the household, region, and family happiness.
Comparisons of institutional and home (informal or formal) care showed that an individual's age had a negligible effect on the probability of selecting institutional care over home care. In addition, as age increased, individuals preferred formal care at home to informal care. Although other studies support these findings,17,20) other studies reported conflicting findings.13,18) It is most likely that patients would prefer to avoid being a burden to the family. In other words, older people may be more concerned about this issue, making them more likely to choose formal care.36)
Men were less likely to select formal care (institutional or formal care at home) compared to women. Instead, they preferred to receive informal care at home. The traditional family structure in Turkey is patriarchal, and domestic work, including when caring for the aged and children, is generally perceived as the duty of women. Throughout their lives, men are generally supported by women in their families, including mothers, sisters, and spouses. Therefore, men are more likely to prefer informal care at home when they are older.
Regarding marital status, divorced individuals were almost 10% more likely to select institutional care compared to single individuals, while widowed individuals were almost 10% less likely to select institutional care over home care. Among home care options, all marital categories (married, divorced, widowed) were less likely to select formal care at home than single individuals. Fernandez-Carro15) also reported that widows more often preferred co-residence over institutional care. These may relate to the fact that divorced or single individuals may choose to live independently, i.e., without the presence and support of a spouse. However, living without a spouse was not the choice of widowers. This type of choice may also affect future preferences.
Individuals with higher educational levels were more likely to select institutional care over home care. Additionally, we observed a clear trend in which more educated individuals were more likely to prefer formal care at home over informal care. This finding was confirmed by Liu et al.,20) indicating that more educated people more often preferred institutional care, and some studies state that less educated people prefer home care more.6,10) This finding can be explained by the fact that people with higher education have different ideologies and are more open to accepting innovations.20) Individuals with a higher level of education also likely have higher income levels, implying that they may have better opportunities to receive formal care. Moreover, their knowledge of LTC services is better than that of their less-educated counterparts. Therefore, they may be more likely to receive LTC services from professionals compared to less-educated individuals.
Individuals with extended or elementary families were almost 5% less likely to select institutional care compared to single individuals. In terms of home care, the same group was less likely to prefer formal care over informal care. This confirmed the literature suggesting that more informal support and wider social networking (e.g., more frequent contact with children and relatives) increased the preference for informal and mixed assistance over institutional care.40) Not only the family type but also the characteristics of the individual's location (like the city center or district) and the region in which an individual lived affected the LTC preference. Accordingly, individuals living in city centers and districts are almost 5% more likely to select institutional or formal care at home compared to their counterparts living in villages. This can be explained by the tight relationships between kinship and neighborship in the villages, in contrast to the decrease in social solidarity in the cities.
People living in the above-mentioned regions were more likely to select institutional care compared to individuals living in Eastern Anatolia, which has the lowest levels of development and education in Turkey.41) In addition, the family structure is more extensive and the number of children in families is comparatively high, implying that the traditional family culture remains strictly maintained in Eastern Anatolia. In contrast, the levels of development and education are comparatively high, family sizes are relatively small, and the number of children is proportionately low in the Mediterranean, Aegean, and Marmara regions. The variations in these characteristics may be associated with differences in LTC preferences.
Individuals living in flats were more likely to prefer institutional or formal care at home than their counterparts living in houses. The weaker neighborly relationships and accustomization to individual lifestyle of respondents living in flats may be a potential mechanism for this finding.
Individuals with more children were less likely to prefer institutional or formal care at home. This may be related to more informal caregiver opportunities. Having more caregiver opportunities has positive effects, including the ability to distribute the burden of care among potential caregivers. This also affects the caregivers’ willingness to provide care. When the caregiving burden is too high, caregivers such as children or spouses may avoid caregiving.14,42) Hence, sharing the burden or support may affect caregivers’ willingness to provide care.
Although health status does not significantly impact LTC care preferences, increased family happiness is associated with a decreased probability of selecting institutional care over formal or informal care at home. Hong et al.17) suggested that poor health is the main determinant for relocation in older adults. Specifically, individuals with poor health status are more likely to relocate to a nursing home.17,43) Nonetheless, we observed no significant effects of health status on LTC preference in the present study, confirming the findings of Liu et al.20) However, the observed effect of happiness confirmed the suggestion by Sugimoto et al.18) that a good family relationship affects preference for home care over institutional care. It is reasonable that individuals want to live with their loved ones, especially when they become frail due to aging.
The extended family type, which was formerly common in Turkey, has been replaced with smaller families in recent years. Increased job opportunities in major cities have led young people to migrate from rural areas to cities. Furthermore, women's participation in the labor force has increased, implying their decreased roles as family caregivers. Socio-demographic transitions in recent years have affected lifestyles and may result in the tendency towards an individual lifestyle from the traditional family structure. Despite this, the traditional family structure is preserved, especially in rural areas. This is also true for LTC preferences. Hence, it is important to consider the current and future sociodemographic status of the society when designing LTC systems.
Approximately seven of ten people in Turkey prefer to receive care in their own homes, while more than half of these seven prefer to receive care from their family members. While other studies worldwide have also reported a higher preference for home care,11,15,25) some studies have suggested a change in preferences over time. Two studies conducted 7 years apart reported an increased preference for institutional care in China, although the preference for home care remained very high, at 80%–90%.20,44) The preference for institutional care in Japan is almost 40%, with more young people preferring institutional care.13,18) This implies that more individuals may benefit from institutional care in Japan in the future. The preference types for care and service use are also influenced by government incentives. For example, as a result of a policy encouraging home care in Germany, 80% of those who benefit from LTC services receive home care.45)
Socio-economic, cultural, and policy differences among countries are evident in LTC preferences and practices. Although no uniform LTC system is applicable to every country, the experience of each country is valuable and can guide other countries in designing their own LTC systems. Therefore, it is important to identify the preferences for LTC in Turkey, a society that has transformed from a traditional family structure to a nuclear family, where internal migration is experienced due to wider employment opportunities and in which the role of women in society has changed. Our findings revealed that informal care remains the predominant preference for individuals in Turkey. Age, sex, education level, marital status, family type, number of children in the household, region, and family happiness were significantly associated with preferences for LTC. Individuals' preferences should be strengthened according to their preferences, taking regional differences into account.
Since the predominant preference is for informal care, the government should develop policies to train caregivers and support them financially, socially, and emotionally. Examples of good practices in different countries, such as free training and consultancy services, the possibility of benefiting from temporary institutional or formal care, care payments, insurance, and pension rights for informal caregivers, can help inform this development.
This study has several limitations. First, the study was cross-sectional; thus, causal conclusions were not possible. Second, because the survey data were self-reported, they may have been biased. Third, some regulations were set for the LTC system in Turkey after the survey was conducted in 2016. For instance, receiving services from daycare centers could not be considered an option in the present study. However, the positive effects of daycare centers on both the care recipient and caregiver have been reported.46) Thus, these services may support individuals needing to live longer in their homes.47) Although these changes may have influenced the preferences in favor of informal care, no alternative dataset is available to avoid this issue. Future studies that consider daycare centers as an alternative may contribute to the existing literature.
In conclusion, although individuals preferred informal care, some socio-demographic factors positively affected institutional care preferences. However, no LTC insurance exists in Turkey and the degree of dependency or income status before receiving services are barriers to LTC. These barriers affect an individual's ability to choose freely. Preferences may shift when the barriers to access care are removed and the variety of services is increased. In this context, our study provides valuable evidence that can contribute to developing an LTC system in Turkey. However, further studies are needed to assess LTC practices recently implemented in Turkey and show any changes in individuals' preferences over time.
Notes
We would like to thank Prof Heinz Rothgang and Prof Lorraine Frisina Doetter from SOCIUM (Research Center on Inequality and Social Policy) at Bremen University. This work was financially supported by TUBITAK (The Scientific and Technological Research Council of Turkey) under the International Post-doctoral Research Fellowship Programme. Data gained from Turkey Family Structure Survey performed by TurkStat.
CONFLICT OF INTEREST
The researchers claim no conflicts of interest.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization, OG, HGA; Data curation, OG; Investigation, OG; Methodology, HGA; Writing–original draft, OG, HGA; Writing–review & editing, OG, HGA.