Fear of Falling and Environmental Factors: A Scoping Review
Article information

Abstract
Fear of falling is a geriatric condition that must be understood from both a clinical perspective and from the environment in which older adults live. This review aimed to describe the scientific evidence reported in the last 5 years regarding the fear of falling in older adults and its relationship with environmental factors. The relationships between fear of falling and environmental factors are mainly evidenced in the built environment. Older adults with a fear of falling are described as perceiving the built environment as dangerous when they do not meet the requirements of safety, accessibility, and comfort; they also report the importance of living in communities with controlled crime levels and available social support for older adults to improve their insecurity and feelings of vulnerability.
INTRODUCTION
Fear of falling is a geriatric condition that has been described as both a cause and a consequence of falls.1) This condition is defined as the loss of confidence to avoid falls while performing relatively non-hazardous daily activities so that the person avoids performing them despite having the capabilities to do so.2,3) The prevalence of fear of falling ranges between 3% and 85% and varies among populations, partly due to the diversity of methods used for its measurement.4) As fear progresses, the person restricts the performance of activities inside and outside the home, increasing the likelihood of further mobility restriction,5,6) which contributes to a cycle of inactivity and deconditioning, with a loss of postural control, in addition to functional limitation, mobility disability,7) increased risk of falls,8) and, ultimately, institutionalization.9) Fear of falling involves physical, cognitive,10) and psychological components,10,11) which do not necessarily overlap; its predictors have been well studied from the individual aspect, with the physical and functional components being the most investigated. A loss of postural control,12-14) functional impairment,15) mobility disability,16,17) visual and hearing impairments,18) and a history of falls8) are predictors of fear of falling. Regarding the cognitive component, the fear of falling is associated with decreased executive functions, decreased memory, verbal fluency,19) and increased time to perform dual tasks.20) Concerning the psychological component, depression is a predictor of fear of falling,11,21) and emotion regulation, fear of falling, and fear-related avoidance behavior are correlated.22) Other conditions that predict fear of falling are age,16) being female,16,17) poor self-perception of health,16,21) and polypharmacy.21)
Regarding the environment, most studies have evaluated the influence of the built environment as a variable that influences mobility and disability in older adults, in which the aesthetics of the built environment and the combination of land use and access are predictors of increased physical activity in this population.23) Likewise, a combination of neighborhood attributes is significantly related to physical activity. Residential density,24) commercial destinations, transit stops, and sidewalks are associated with increased compliance with physical activity guidelines, while neighborhoods that are highly walkable but unsafe and with few recreational facilities show higher compliance with total physical activity guidelines.25) In contrast, older adults living in neighborhoods with low socioeconomic conditions, residential instability, and negative street characteristics show a higher prevalence of physical disability and difficulty in leaving the home.26) Some studies have also identified characteristics that negatively affect the mobility and physical activity of older adults from the perspective of the environment. However, few studies have reported on the relationship between fear of falling and the environment, a necessary topic as this geriatric condition directly affects mobility.
This review focuses on the relationship between the fear of falling and the environment in which older adults live. It is important to identify whether the characteristics of the environment contribute to the presence or progression of fear of falling, as occurring with physical activity or the presence of a disability. Assessment of the fear of falling should be approached not only from a clinical perspective but also from other sectors that accompany and guarantee the preservation and improvement of health in groups of older adults. Moreover, the development of intersectoral interventions requires the identification of the environmental attributes that most influence the fear of falling.
According to the World Health Organization (WHO), healthy aging involves creating environments and opportunities that enable people to be and do what they value throughout their lives. Therefore, a better understanding of how people interact with their environment and to what extent the environment hinders or enables their functional capacity is required. In this sense, the healthy aging model argues that the adaptation of older adults to their environment requires understanding and interventions related to geriatric conditions from the following five areas or factors: the built environment; people and their relationships; attitudes and values; health and social policies; the systems that support them and the services they provide.27,28)
In this context, the objective of this review is to describe the scientific evidence in the last 5 years regarding older adults with a fear of falling and the relationship of this condition with environmental factors according to the model of healthy aging.
LITERATURE SEARCH
We conducted a review based on the parameters of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.29) We searched the Scopus, Web of Science, and PubMed databases. The search in the Web of Science and PubMed used the keyword “fear of falling” initially, with refinement using Boolean (AND) and specific descriptors such as “environment, build environment, family relations, social relations, attitudes, health policy, public policy, health services, factors a scoping review intervention.” We conducted this search between January and April 2021.
The inclusion criteria were quantitative and qualitative studies of any design and scope focused on environmental components (housing, neighborhood, and city) and fear of falling in older people and manuscripts published in English between 2016 and 2021. We excluded articles that described the environment and fear of falling as independent covariates and those that only mentioned them as related aspects without measurement.
We identified a total of 143 articles. A reviewer assessed these studies to eliminate duplicates and select those eligible for analysis. After 21 duplicate records were eliminated, there were 126 articles for screening based on the titles and abstracts, of which 99 were eliminated because the variables of interest did not meet the inclusion criteria. Subsequently, full-text analysis was performed on the remaining 27 articles and 10 were excluded because the variables of interest in the present review were independent covariates or aspects related to the topic but without measurement. Finally, we included 17 articles in the analysis. Fig. 1 illustrates the study selection.
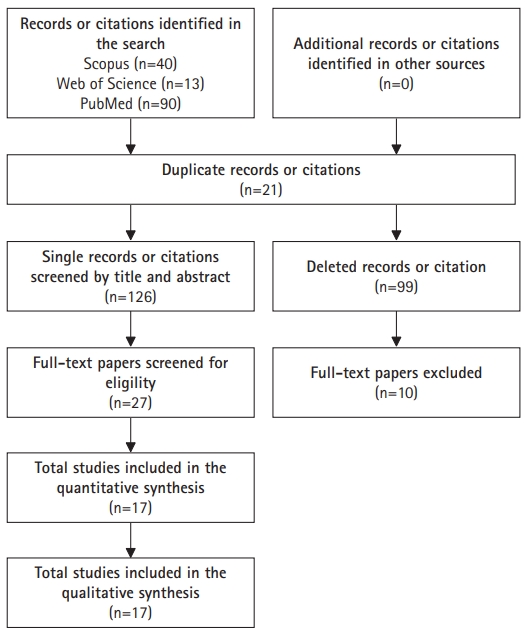
Information flow diagram for the different phases of the review.
Data Extraction
For the analyses, we extracted data on sample size, sociodemographic characteristics (age and sex), study type (cross-sectional, longitudinal, or experimental), and environmental dimensions from the perspectives of healthy aging (the built environment; people and their relationships; attitudes and values; health and social policies; and the systems that support them and the services they provide).27,28,30)
RESULTS
Study Characteristics
The 17 studies included in the analysis had a total sample of 2,901 participants; the average participant age was 72±6 years, 59.9% of whom were female and 40.1% were male. Among the included studies, 58.8% (n=10) were cross-sectional, 11.8% (n=2) were clinical trials (CT) (one explanatory and one pragmatic CT), 5.9% (n=1) were longitudinal studies, and 23.5% (n=4) were qualitative studies. The characteristics of the quantitative studies and their measurements and interventions with respect to the environment are presented in Tables 1 and 2. The characteristics of the qualitative studies and identified topics are listed in Table 3.
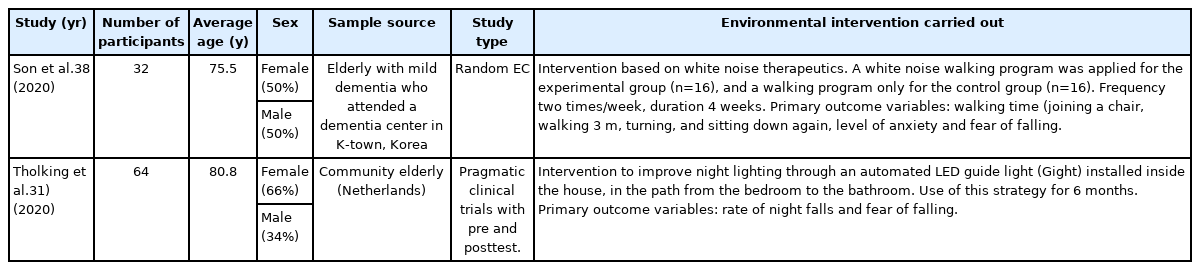
Clinical trials included in the analysis

Cross-sectional and longitudinal studies included in the analysis
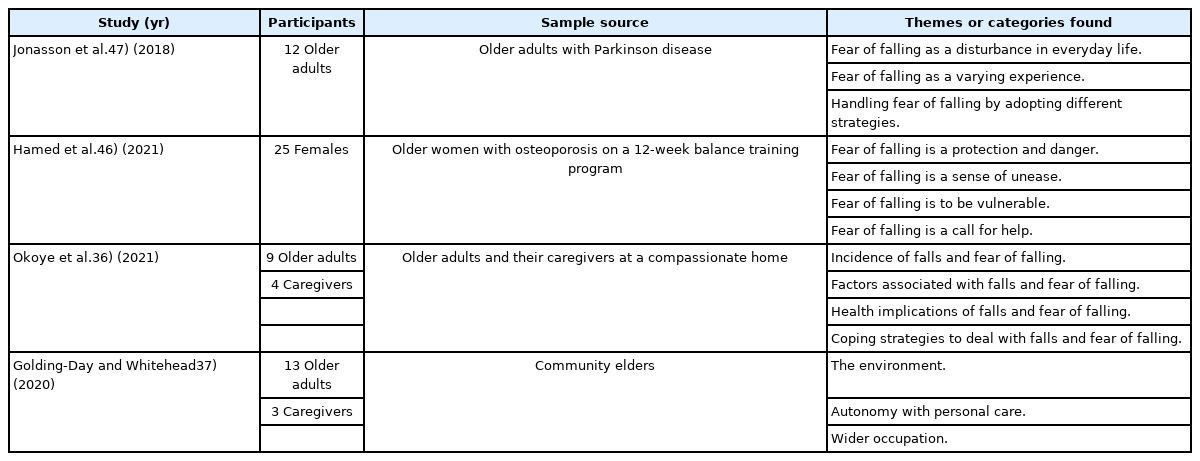
Qualitative studies included in the analysis
Study Quality
The results of the present review showed that most of the studies were cross-sectional; thus, the level of evidence was low. However, explanatory multivariate analysis predominated in eight of the studies, which performed linear and logistic regressions. The single longitudinal study used latent class analysis, while the two CTs reported results based on per-protocol and intention-to-treat analyses. Only two studies reported correlational findings. All studies used valid outcome measures and the analyses were adjusted for key sociodemographic and clinical variables.
RELATIONSHIPS BETWEEN FEAR OF FALLING AND THE ENVIRONMENT
The results showed that most of the studies assessed or provided interventions for factors related to the “built environment,” namely, the home, neighborhood, and city. A smaller number of studies described the fear of falling and the perception of social support and safety; their results showed an approach to factors related to “people and their relationships.” Likewise, studies also mentioned “attitudes” regarding concern about falling among older adults. No specific results were identified with respect to the other factors mentioned in the healthy aging model.
Fear of Falling and Factors Related to the Built Living Environment
Only one pragmatic CT demonstrated the results of a modification of the living environment. The authors assessed the effectiveness of nighttime automated LED lighting on the path from the bedroom to the bathroom31) in reducing the fear of falling and improving sleep in older adults. Intention-to-treat analysis showed a significantly decreased nighttime fear of falling, from a score of 5.5±3.0 to 3.8±3.2 (on a 1–10-point scale) at the end of the study (z=-3.31, p=0.001, r=0.30). Per-protocol analysis yielded similar results, with a decrease from 5.6±3.1 at baseline to 4.0±3.4 at final assessment (z=-2.41, p=0.016, r=0.26). Additionally, the mean scores on the Falls Efficacy Scale International (FES-I) scale also improved significantly, from 36.9±12.9 at baseline to 31.5±11.8 at the final evaluation (z=-2.69, p=0.007). Likewise, 57% of the participants reported a subjective decrease in their fear of falling, with a high appreciation of the use of this innovative strategy (8.4±0.8 on an appreciation scale of 0–10).
In contrast, three cross-sectional studies evaluated the relationship between the fear of falling and environmental hazards within a dwelling. First, they applied a home safety checklist and showed that the greatest fear of falling was associated with walking on a slippery surface, while the lowest fear was associated with getting dressed or undressed. Likewise, the use of inappropriate footwear, slipping on uneven surfaces, and reaching objects in high places showed the highest mean scores in people with a fear of falling. A significant relationship was observed between housing safety status, prevalence of falls, and fear of falling (p<0.0001).32) A second study showed similar results regarding demanding physical activities reported by hypertensive older adults and the intensity of their fear of falling, including walking on slippery surfaces, walking on uneven surfaces, walking up or down a slope, climbing or descending stairs, reaching for an object or bending, and taking a bath or shower.
The fear of falling is also higher when hazards are present in the environment of older people; for instance, the fear of falling is significantly higher than that in individuals living in safer places (p=0.001).33) The third study applied an instrument to identify hazards in housing, which showed a higher frequency (30%) in toilet and bathroom areas (no grab bar, no non-slip mat, distant toilet), slippery floors, housing without access to headlights, and inadequate footwear. Binary logistic regression analysis of the total score of the instrument showed no significant association with fear of falling (Exp(β)=1.010, p=0.694); however, further analysis of the instrument subscales showed a lower probability of association between a high fear of falling and housing hazards (p=0.023) and higher with functional problems (p<0.001). Neither domain (environmental hazards and functional problems) was associated with activity restriction due to a fear of falling.34)
Concerning the barriers around the home and their relationship to the fear of falling, one study evaluated the perceived level of outdoor qualities in older adults who were classified as frequent and infrequent users of hallways and outdoor living areas. The researchers asked the participants about the design quality, physical comfort, and their perceived satisfaction with such areas. The results showed a greater fear of falling among individuals who were not frequently outdoors (odds ratio [OR]=0.597, p=0.023 for infrequent outdoor use and OR=0.418, p=0.003 for frequent outdoor use), as well as a low perceived level of the general design qualities of the outdoor areas and comfort when using these areas (OR=0.522, p=0.004 for infrequent users and OR=0.414, p=0.002 for frequent users). Additionally, adequate corridor design (OR=0.614; 95% confidence interval [CI], 0.405–0.931), comfort levels in the use of outdoor areas (OR=0.657; 95% CI, 0.437–0.989), and frequency of use of outdoor areas (OR=0.538; 95% CI, 0.368–0.787) were associated with a decreased fear of falling outdoors after adjusting for individual factors (age, sex, health status, history of falls, vision impairment, and mobility aids).35)
Finally, two qualitative studies described the environmental factors associated with a fear of falling; one study reported a greater fear of falling among older adults in assisted living facilities reported with poor nighttime lighting and poor ambulatory surfaces in their housing.36) A second qualitative follow-up study evaluating the results of adaptations made to older adults’ bathrooms showed that, at 23 months, older adults reported that they continued to use their walk-in shower without any difficulty; they noted that this adaptation had reduced the hazard and led to a larger and safer space with less fear of falling or injury. Similarly, the new bathroom reduced the physical burden on caregivers to assist with bathing, which led to better self-care and autonomy.37)
Fear of Falling and Factors Related to Neighborhood Built Environment
Among the factors related to neighborhood environment, a randomized CT assessed the effects of an intervention based on white noise therapy and walking on walking time, anxiety, and fear of falling in older adult patients with mild dementia. The intervention aimed to block external sounds to reduce the detection of ambient noise and disperse other noises in an irregular and open space, allowing individuals to focus on and detect specific sounds and more efficiently perform activities and tasks. The results showed a decrease in the fear of falling in both groups (experimental group, walking plus white noise; control group, walking only), with a significant difference in the experimental group with a confidence level of 99% (p<0.01) and an 11.5-point decrease compared to the control group.38)
In contrast, a longitudinal study evaluating outdoor mobility trajectories in vulnerable older adults showed four latent trajectories: those with low mobility frequency, high mobility, decreasing mobility over time, and those who did not go outdoors regularly (homebound). Compared to those who frequently went outdoors in a typical week, older adults who never went out tended to have more difficulty walking and a fear of falling; moreover, older adults with a fear of falling were almost four times more likely to be housebound compared to older adults who went out more frequently (OR=3.55; 95% CI, 1.91–6.59) and also showed a higher probability of older age (OR=1.92; 95% CI, 1.25–2.97). Similarly, approximately 14% of respondents lived in a block with mixed land use, 24% had barriers at their home entrance, and the mean sidewalk accessibility score was 3.5±1 on a scale of 0–6.39)
Five cross-sectional studies reported an association of fear of falling with neighborhood aspects such as living in a neighborhood with many broken sidewalks, drainage ditches, presence of strangers,35) worse perceived accessibility and neighborhood conditions,40) living near places with garbage accumulation and/or places with open sewers,41) living in places with high crime rates, and low social support.42,43) In contrast, Lee et al.44) reported a lower likelihood of fear of falling in older adults who perceived that their neighborhoods had well-lit streets, well-maintained streets, and low traffic speed (OR=0.324; 95% CI, 0.162–0.646). Likewise, Lee et al.43) described a lower fear of falling in adults living near supermarkets, stores or free markets, commercial businesses, bus stops, parks, plazas, walking tracks, bike lanes and/or sports courts, and outdoor gyms, as well as those living in places with sidewalks on most streets, with level streets, and those considered safe for walking during the day and at night; as well as those residing near a bus stop, and having an outdoor gym and safe places to walk.
Fear of Falling and Factors Related to the City Built Environment
Only one study addressed this category. This study assessed fear of falling and mobility in the living spaces of five cities with significantly different socioeconomic and cultural characteristics in middle- and high-income countries. The results demonstrated that fear of falling was related to mobility in living spaces and that the strength of the association differed between cities. Before adjusting for confounders, the relationship between the fear of falling and living space was significant for the overall sample of the five cities. After adjustment, the relationship remained significant for three of the five cities; in the other two sites, this association was weak and was explained mainly by functional and clinical factors. In these two cities, the scores were significantly worse, physical environmental barriers were more common, and older adults in these sites required high functional reserves to overcome these barriers and prevent their living spaces from shrinking with age. Additionally, the authors explained that these people lacked the financial means to compensate for the effect of environmental challenges on their living spaces; thus, they relied mainly on their functional reserves.45)
Fear of Falling, People, and their Relationships
Five studies evaluating aspects related to neighborhood social support and safety reported significant differences between the perception of high social support and reduced fear of falling (OR=0.842; 95% CI, 0.772–0.919). These studies defined social support as the cumulative effects of the existence of close relatives, friends/neighbors, and visits received by people other than cohabitants in the last month.43) These characteristics were more significant in individuals with a history of falls. A second study reported that the likelihood of having a fear of falling outdoors was almost two times that of those who perceived that their neighborhood had many strangers (OR=2.520; 95% CI, 1.238–5.129).44) In contrast, another study found that the perception of safety from crime influenced physical activity in frail older adults and that the fear of falling was a mediating factor in the relationship between safety from crime and physical activity.42) Likewise, a study reported that older adults living in places with high crime rates were more likely to report fear of falling (OR=2.62; 95% CI, 1.50–4.56).41) Finally, qualitative studies indicated that a fear of falling involved difficulty spending time with friends and family due to constant worry about falling and an inability to engage in joint activities due to loss of self-confidence.46)
Fear of Falling, Attitudes, and Values
Four qualitative studies reported on attitudes regarding the fear of falling; these studies revealed behaviors or predispositions such as feeling ashamed of public stigmatization due to falling in front of an acquaintance. Fear of falling was seen as a dichotomous condition that protected against harm since it generated a greater awareness of the dangers of the environment and cautious behaviors; moreover, potential danger manifested in a feeling of discomfort owing to the lack of control of such dangers. Thus, slippery surfaces, snow, or rain were reported as the greatest risks for falls and generated greater concern and fear of consequences.46) In contrast, two studies reported that adults with a fear of falling felt vulnerable due to the feeling of aging, awareness of falls, and disability symptoms that led them to perceive danger in everyday environments.46,47)
Another qualitative study reported an unwillingness to accept age-related changes in physical capacity, poor disposition towards walking aids, and misconceptions about falls and fear of falling as inevitable situations that cannot be controlled by the person himself/herself, but rather by spiritual forces. This study also identified caution and greater care to perform activities, as well as avoidance of activities when fear of falling is present.36)
DISCUSSION AND CONCLUSION
When analyzing the results from the environmental factors contemplated in the healthy aging model, results were found for three of them. In the first instance, it can be said that most of the studies evaluated factors related to the built environment, specifically the home and neighborhood. A second aspect is that which shows the relationships of the older adult with his or her family and community; however, only some results are described from the perception of support and social security in the neighborhood. Third, we identified some results related to the attitudes of older adults about a fear of falling. We did not identify studies on the fear of falling and health policies, systems, or services provided.
As the built environment was the main component identified in this review, it is necessary to comment that its measurement is diverse depending on the interests of the authors. In this sense, four studies evaluated or performed intervention of aspects related to the housing environment through validated scales or checklists.31,32,35,48) On the other hand, six of these studies were dedicated to measuring or intervening aspects of the neighborhood environment through various instruments assessing perception in terms of discomfort, accessibility, or use of different neighborhood elements.35,38,40-42,49) Finally, three studies that assessed both aspects of the built environment (home and neighborhood) using different instruments were identified.33,39,45) This can be explained by the fact that the built environment has been addressed from environmental gerontology by different disciplines and theoretical perspectives through disability models,30) neighborhood models,50) land use,51) and person-environment adjustment,52) among others. However, most of the studies analyzed in this review did not specify the theoretical perspective underlying their work.
The main results of studies on the built environment showed that poor lighting, irregular or slippery floors, bathrooms and showers without grab bars, the presence of stairs, and objects in high places were the factors most related to the fear of falling. Likewise, home exterior design was of vital importance for older adults to decide to use it frequently. People with a fear of falling do not go out frequently in the house with exteriors that are considered unsafe or uncomfortable. This is an important aspect to consider, as adults with a fear of falling who do not go outdoors are four times more likely to be confined and have difficulty walking.39) Among the characteristics of the neighborhood environment, irregular sidewalks, poor street lighting, garbage, noise, and poor accessibility to places of commerce, are perceived as unsafe factors for mobility in adults with a fear of falling. As the built environment is a space that has been planned, shaped, and used to meet the needs of daily life,51) neighborhood characteristics can greatly affect the life and health of individuals, influencing their decisions, the risks to which they are exposed, and the resources they can access.
A higher frequency of fear of falling has been reported among older adults in neighborhood environments compared to home environments. Deshpande et al.53) attributed this difference to greater demands to control balance and maintain stability in the neighborhood environment so that the fear of falling in the neighborhood environment may precede that in the home environment. Likewise, people who express fear of falling inside the home, in general, have a lower functional capacity than those who experience a fear of falling only related to activities in the neighborhood.
Environmental gerontology has shown that built environments of the home and neighborhood are particularly important for the functional health and well-being of older adults54,55); however, the specific predictors of the built environment that influence the onset or progression of the fear of falling have not been identified. Therefore, it is important to continue investigating this subject, as the WHO has proposed strategies to achieve age-friendly environments through compliance with a set of basic indicators that include the physical and social environment. Among these indicators is the accessible physical environment, assessed through quality of life in the neighborhood, ease of walking, accessibility of public spaces and buildings, accessibility of public transport vehicles, accessibility of public transport stops, and accessibility of housing.56)
In contrast, studies have reported a negative correlation between the perception of social support and fear of falling,43) while the perception of an unsafe neighborhood or one with many strangers increases the probability of fear of falling in older adults.44) Thus, fear of falling acts as both an outcome variable derived from poor safety and a mediating factor between the presence of delinquency and the performance of physical activity.42) The World Report on Aging and Health27) described the importance of older adults being able to create and maintain relationships as a fundamental aspect of the environment in which they live. The relationships they establish with children, partners, family, friends, neighbors, colleagues, acquaintances, and the community, in general, generate feelings of trust and belonging to certain groups that can provide support and contribute to well-being. Based on this concept, the results of the present review only show some existing relationships between older persons and their community environment; therefore, this knowledge also warrants attention from empirical evidence.
Regarding the attitudes of older adults, the qualitative results of this review illustrated some ways by which older adults react to a fear of falling and identified signs of embarrassment, vulnerability, dual sensations of danger/protection, poor disposition to walking aids, and erroneous thoughts about possible ways of addressing concerns about falling. These aspects are important to consider when developing interventions to avoid or reduce the fear of falling. Likewise, these attitudes must be investigated and validated from a quantitative perspective to provide generalizable results that contribute to the profile that characterizes a person with a fear of falling.
Finally, all the included studies evaluated individual covariates (age, sex, comorbidities, hospitalizations, presence of falls, physical capacity, visual acuity, polypharmacy, perception of health status, etc.) as mediating aspects between the presence of a fear of falling and the environment. Kakhki et al.33) reported that people with functional problems had a higher probability of presenting a high degree of fear of falling within the dwelling. Likewise, Lee et al.35) showed that comfort levels in outdoor living areas and their frequency of use were associated with a decreased fear of falling after adjusting for individual factors such as age, sex, health status, history of falls, vision problems, and use of mobility aids. These findings demonstrated the importance of considering individual variables when evaluating the relationship between the fear of falling and the environment as conditions that cannot be seen in isolation, given the variability in the aging process. Thus, the same environment can have different effects on individuals.57)
In conclusion, our results confirmed that the relationships between the fear of falling and environmental factors are mainly evidenced in the aspects of the built environment. The evidence supporting these relationships was derived from cross-sectional studies that have mostly performed multivariate analyses, taking into account mediating covariates related to intrinsic capacity (especially physical and functional aspects). Older adults with a fear of falling are characterized by perceptions that the built environments are dangerous when they do not meet the requirements of safety, accessibility, and comfort, as well as the importance of living in communities where crime levels are controlled and where social support is provided to older adults to improve their insecurity and feelings of vulnerability.
The limitations of this review include the lack of generalizability of the results regarding the relationships between the fear of falling and the environment owing to the level of evidence. Likewise, it is difficult to make conclusion regarding environmental factors because different studies have approached this concept from different theoretical perspectives and paradigms.
Notes
CONFLICT OF INTEREST
The researchers claim no conflicts of interest.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: CLVR; Data curation: CLVR, CLC; Investigation: CLVR; Methodology: CLVR; Supervision: CLC; Writing-original draft: CLVR; Writing-review & editing: CLC.