INTRODUCTION
The proportion of the geriatric population in society is gradually increasing. According to a World Health Organization report, the number of people aged ≥60 years, which was one billion in 2020, is expected to increase at an unprecedented rate to 2.1 billion by 2050.1) National data reveal that the older population will double by 2060.2) With an increase in the geriatric population, geriatric syndromes are of increasing importance. Geriatric syndromes are common, complex, and costly health conditions in older individuals.3) Sarcopenia, which causes physical disability with a progressive and generalized decrease in skeletal muscle strength and mass, is also defined as geriatric syndrome.4)
In general, 5%–13% of people aged 60–70 years and 11%–50% of people aged ≥80 years have sarcopenia.5) A systematic study, reported sarcopenia in at least one of 20 members of the community, with the incidence increasing to up to one in three in frail older individuals.6) Sarcopenia is associated with many clinical consequences such as falls, fractures, physical disability, and increased mortality, causing high personal, social, and economic burdens.7) Sarcopenia is also associated with many chronic and endocrine comorbidities such as diabetes mellitus, depression, and cardiovascular diseases. However, the relationship of sarcopenia with cognitive function remains unclear.8) Sarcopenia and cognitive disorders share many co-occurrence mechanisms, which has prompted researchers to investigate the relationship between cognitive and motor/physical functions.9)
In this context, the present study investigated the relationship between sarcopenia and cognitive function in older adults.
MATERIALS AND METHODS
Study design and participants
This study included 201 participants aged >65 years at Department of Family Medicine, the Health Sciences University Kartal Dr. Lutfi Kirdar City Hospital, Istanbul, Turkey, between July 1, 2020, and January 31, 2021. The Kartal Dr Lutfi Kirdar City Hospital Clinical Research Ethics Committee approved this study (No. 2020/514/180/33). Informed consent was obtained from all participants at the beginning of the study. This study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.10)
We calculated the sample size for a known population with an unknown prevalence within the 95% confidence interval. We evaluated all participants and collected data on their anthropometric measurements. The same examiner performed all measurements. Body mass index (BMI) was calculated as body weight (kg)/height squared (m2). Body analyses of the patients were performed using an Omron Karada Scan device on an empty stomach, without metal, and with bare feet.
Sarcopenia assessment
Sarcopenia was diagnosed according to the European Working Group on Sarcopenia in Older People (EWGSOP2) criteria.3,4) We also screened all patients based on the SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire. We considered participants with a SARC-F total score ≥4 to be at risk for sarcopenia.11) The handgrip strength of patients with sarcopenia risk was evaluated using a Baseline Digital Smedley hand dynamometer. We asked the participants were asked to keep their elbows close to the body, flex the elbow to 90°, and grasp the dynamometer and squeeze as hard as possible. We used the highest value of three measurements for analysis. We defined probable sarcopenia as handgrip strength <27 kg in male participants and <16 kg in female participants.3,4)
We applied bioelectrical impedance analysis (BIA) to evaluate the skeletal muscle masses of participants with probable sarcopenia. Jannsen et al.12) defined skeletal muscle index (SMI) as the percentage of total body mass (skeletal mass/body weight x 100), and expressed SMI% in units. A low SMI was considered normal if it was greater than one standard deviation from the sex-specific mean for young adults (18–39 years) based on data from the Third National Health and Nutrition Examination Survey (NHANES III). Patients with values one standard deviation below the mean were defined as having sarcopenia. The present study used cutoff values of <37% (for male) and <27.6% (for female), with participants with values these cutoffs categorized as having sarcopenia.3,4)
Cognitive function
We used the Standardized Mini-Mental Test (SMMT) and Standardized Mini-Mental Test for the Untrained (SMMT-E) to evaluate the cognitive status of the participants. Participants who correctly completed all test areas received the maximum total score of 30. We defined normal cognitive function as scores of ≥24 points, mild dementia as scores of 18–24, and severe dementia as scores ≤18.13,14)
Statistical analysis
Study data were analyzed using IBM SPSS Statistics for Windows, version 21.0 (IBM, Armonk, NY, USA). Descriptive criteria (frequencies, percentages, means, medians, standard deviations, and minimum-maximum values) were reported. We applied Kolmogorov-Smirnov tests to assess normality. Pearson and Spearman correlation tests were used to evaluate the relationships between continuous variables. Chi-square test was used. Statistical significance was set at p<0.05.
RESULTS
This study included a total of 201 participants—44.3% (n=89) male and 55.7% (n=112) female. The mean age of the participants was 73.3±6.0 years. Most the participants were married (69.2%; n=139), high school graduates (29.4%; n=59), and retired (61.7%; n=124). The mean BMI was 27.9±4.1 kg/m2. According to BMI classification, approximately half of the participants (46.8%; n=94) were overweight. The general characteristics of the participants are presented in Table 1.
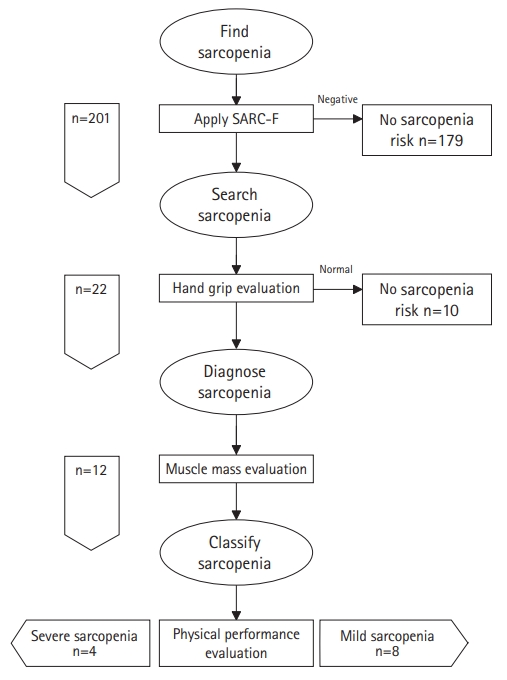
In this study, 10.9% (n=22) of the participants were at risk for sarcopenia. To confirm the diagnosis of sarcopenia, we evaluated the participants’ muscle mass and handgrip strength, which showed that 6.0% (n=12) of the participants had definite sarcopenia. The results of walking tests to assess the sarcopenia severity revealed severe sarcopenia in 33.3% (n=4) of the participants (Fig. 1).
Examination of the relationship between demographic data and sarcopenia status showed a significant difference between the presence of sarcopenia and age. In this study, 16.7% (n=2) of participants with sarcopenia were aged ≥85 years compared to 3.2% (n=6) of participants without sarcopenia (p=0.041). We observed no significant differences between other demographic characteristics and sarcopenia (Table 2).
Evaluation of the cognitive functions of the participants using SMMT showed a mean SMMT score of 26.2±3.3. While 80.6% (n=162) of the group had a normal cognitive function, 19.4% (n=39) showed impairment. Our examination of the association between cognitive impairment and SARC-F revealed that 8.6% (n=14) and 20.5% (n=8) of participants with normal cognitive function and cognitive impairment, respectively, were at risk of sarcopenia (p=0.045). We next assessed the relationship between cognitive function and sarcopenia status, finding that 3.7% (n=6) of participants with normal cognitive function were sarcopenic, compared to 15.4% (n=6) of participants with cognitive impairment (p=0.006) (Table 3).
DISCUSSION
This study aimed to determine the prevalence of sarcopenia and investigate the relationship between sarcopenia and cognitive function in older individuals. It was found that 10.9% (n=22) of participants was risky for sarcopenia and that 6.0% of the participants had definite sarcopenia. The rate of sarcopenia was significantly higher in older individuals with cognitive impairment compared to those without cognitive impairment (15.4% vs. 3.7%).
Epidemiological studies on the prevalence of sarcopenia have reported sarcopenia in 5%–13% of people aged 60–70 years and 11%–50% of people aged >80 years.5) Differences in sarcopenia definitions, cutoff values, measurement methods, and formulations have led to different prevalence reports in the literature. BIA underestimates fat mass, overestimates muscle mass, and shows a small margin of error in estimating skeletal muscle mass.15) Kim et al.16) reported sarcopenia frequencies of 14.2% in female and 5.1% in male based on the SMI. The authors also reported different sarcopenia frequencies using different methods to assess muscle mass. In our study, the overall incidence of sarcopenia was 5.9%, while it was 8.0% in female, and 3.3% in male. The frequency of sarcopenia was 25% in participants aged ≥85 years, with a significant association between age and sarcopenia. Given the progressive decrease in muscle mass with age, this result was expected. However, the frequency of sarcopenia in our study was relatively low, even in those aged >85 years. We attribute this finding to the living conditions of the older individuals in this study. Physical inactivity and obesity are important risk factors for sarcopenia. As our study area was an island, the inhabitants have high physical activity levels.
We observed no significant difference in the presence of sarcopenia between sexes. In their meta-analysis including 58,404 patients, Shafiee et al.17) reported a similar prevalence of sarcopenia between sexes, consistent with our findings. The relationship between sex and sarcopenia has been inconsistent in the literature. Some studies reported a higher reduction in muscle mass in male than in female.18,19) Iannuzzi-Sucich et al.20) reported the highest prevalence of sarcopenia (52.9%) in male aged >80 years compared to 31.0% among female of the same age. Various endogenous and exogenous factors determine the prevalence of sarcopenia in both sexes. Hormonal changes that play a role in decreasing muscle mass occur more slowly in male than in female. After the menopause transition, the concentrations of sex steroids containing both estrogen and androgen decrease significantly. The reduction in sex steroids in male is much slower than that in female.21)
In our study, the rate of sarcopenia was significantly higher in older individuals with cognitive impairments compared to those with normal cognitive functions. Ida et al.22) reported a significant relationship between sarcopenia and mild cognitive impairment (MCI) using the Japanese version of the SARC-F in a study of Japanese participants with diabetes. Another study showed that physical performance but no other markers of sarcopenia were independently associated with cognitive impairment.23) Lee et al.24) reported that sarcopenia was associated with MCI in older Korean female. Moreover, a recent meta-analysis showed evidence regarding the relationship between sarcopenia and cognitive impairment.25)
This study is one of a few to assess sarcopenia and cognitive function in the Turkish population. However, our study had some limitations. First, because of the study area, the findings cannot be generalized. The study area was an island near a large metropolis (Istanbul) and the participants had higher socioeconomic status and average life expectancy than those of the general population. Moreover, as motor vehicles are not allowed on the island, the physical movement capacity of the participants was also higher than that of the general population. Additionally, the MMT is a screening tool that cannot diagnose dementia. Finally, the cross-sectional design does not show causality.
In conclusion, the results of our study revealed the frequency of cognitive impairment in older individuals at risk of sarcopenia and/or those diagnosed with sarcopenia. With the rapid increase in the geriatric population, neuropsychiatric diseases have become a critical public health problem worldwide and in our country. The correlation between SARC-F and SMMT findings suggests that patients at risk of sarcopenia can also be assessed for cognitive impairment.