INTRODUCTION
Increased life expectancy and declining fertility have brought about dramatic shifts in the age structure worldwide.1) The number of older adults has increased substantially in recent years in most countries and regions.2) This growth is projected to accelerate in the coming decades. Korea’s population is also rapidly aging. A recent study published in The Lancet showed how life expectancy would change in 35 developed countries by 2030 using data from the World Health Organization.3) According to this study, South Korea is likely to become the first country where life expectancy will exceed 90 years. In 2000, the percentage of population aged 65 years and over accounted for 7% of the total Korean population and this values increased to 14% by 2017.4) Thus, Korea is one of the most rapid countries in terms of the speed of population aging.
According to the Survey of Korean Elderly Status in 2014, about 90% of Korean older adults had more than 1 chronic disease diagnosed by physicians and 46% had more than 3 chronic diseases.5) In general, Korean older adults have 2.6 chronic diseases. In addition, one-third of Korean older adults had depressive symptoms, as assessed by the short form of the Geriatric Depression Scale and an estimated 10% of the total elderly population had dementia in 2016.6)
The increasing number of older adults and the current health status of Korean older adults had led to increased medical expenditure under the National Health Insurance. In 2014, older people comprised 35.5% of medical expenses among National Health Insurance costs.7)
Humans have approximately 642 skeletal muscles and the skeletal muscle mass makes up 40% to 50% of the total body weight. Skeletal muscles have several crucial functions including posture, locomotion, and breathing.8) Regulation of metabolism, heat production, and energy storage are also important functions of skeletal muscles.
The muscle mass progressively decreases after 20–30 years of age. Men have a greater muscle mass than women, but the loss of muscle mass is more rapid in men.9) The loss of muscle mass is associated with a decrease in muscle strength and aerobic exercise capacity. The annual rate of muscle mass decline is about 1%–2% and accelerates to 2%–3% per year after 60 years of age; the rate further increases after the age of 75 years.10) A 2-year study measuring the change in body composition using magnetic resonance imaging (MRI) in elderly African American women demonstrated significantly decreased muscle mass, especially in the lower extremities.11) In contrast, fat mass, especially visceral and intermuscular fat, was increased. The decrease in skeletal muscle mass and the increase in ectopic fat is a common age-related remodeling of body composition.
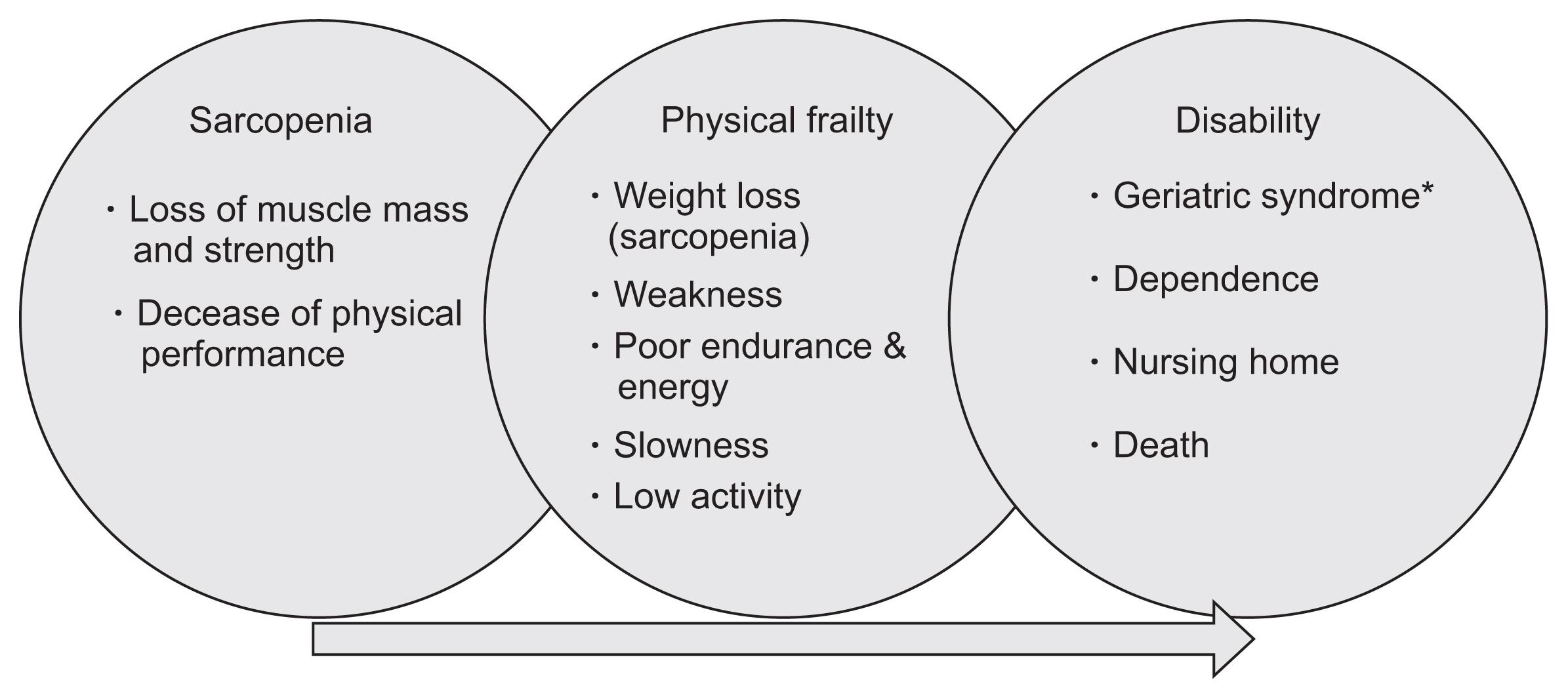
The progressive decline in muscle mass and strength, termed sarcopenia, develops as a consequence of aging.12) Sarcopenia may progress to frailty, loss of independence, physical disability, and increased mortality in older adults (Fig. 1).13–15) Preservation of physical and cognitive function are important in the care of older people. A key strategy is to prevent the functional decline rather than attempting to recover functional loss. The US Centers for Disease Control and Prevention established an International Classification of Diseases, Tenth Revision, Clinical Modification code for sarcopenia, M62.84, which became available on October 1, 2016.16) Thus, establishment of an operational definition for sarcopenia and screening for sarcopenia before functional decline in older adults is urgently required. In this review, I discuss the diagnostic criteria for sarcopenia in Korean older adults.
WHAT IS SARCOPENIA?
The term sarcopenia, sarx for flesh and penia for loss, was first coined by Rosenberg17) in 1988 when he described the age-associated decline of lean body mass. However, many studies indicated that the reduction of muscle strength was more involved compared to muscle loss in health outcomes related to sarcopenia12,18) and that the relationship between strength and mass was not linear.19) In 2010, the European Working Group on Sarcopenia in Older Persons (EWGSOP) defined sarcopenia as a syndrome characterized by a progressive and generalized loss of skeletal muscle mass with either muscle weakness or poor physical performance.12) Several medical organizations subsequently proposed similar conceptional definitions of sarcopenia, such as age-related decrease of muscle mass with limited mobility.20,21) Sarcopenia is associated with a risk of adverse outcomes such as physical disability, poor quality of life, and death. These definitions for sarcopenia better demonstrated its associations with various health outcomes in older adults compared to definitions based only on muscle mass.12,22,23)
HOW TO DIAGNOSE SARCOPENIA?
Baumgartner et al.28) first proposed the appendicular skeletal muscle mass (ASM) divided by height squared (ASM/height2) as a representative muscle index. He suggested the diagnostic criteria for sarcopenia as the ASM/height2 less than 2 standard deviations (SDs) below the mean of healthy young adults (Table 1). The EWGSOP recommended the presence of both low muscle mass and low muscle function (strength or performance) for the diagnosis of sarcopenia.12) Measurements of muscle mass using dual-energy x-ray absorptiometry (DXA) or bio-impedance analysis (BIA), muscle strength by handgrip strength, and physical performance by gait speed or Short Physical Performance Battery were required for the diagnosis of sarcopenia.
As a cutoff point of low muscle mass, the EWGSOP suggested an ASM/height2 less than 2 SD below the gender-specific young reference groups or the lowest quintile of study populations such as the Health and body composition study.28,29) The Asian Working Group for Sarcopenia (AWGS) also proposed diagnostic criteria for sarcopenia in Asian older people by adopting the recommendation of EWGSOP but considering ethnic differences in skeletal muscle mass and muscle strength.30)
Recently the Foundation for the National Institutes of Health (FNIH) Sarcopenia Project suggested new criteria for sarcopenia categorized by muscle mass, muscle strength, and physical performance.31) They proposed a new muscle mass index of the ASM divided by body mass index (BMI).
OPERATIONAL DEFINITION FOR SARCOPENIA IN KOREAN OLDER ADULTS
Kim et al.32) reported a prevalence of sarcopenia in Korean older people (defined by ASM/height2 < 2 SD of healthy young adults) as 9.3% in men and 0.2% in women using data from the 2008–2010 Korean National Health and Nutrition Examination Survey (KNHANES) (Fig. 2). Why was the prevalence of sarcopenia defined by the height-adjusted ASM very low in Korean older women?
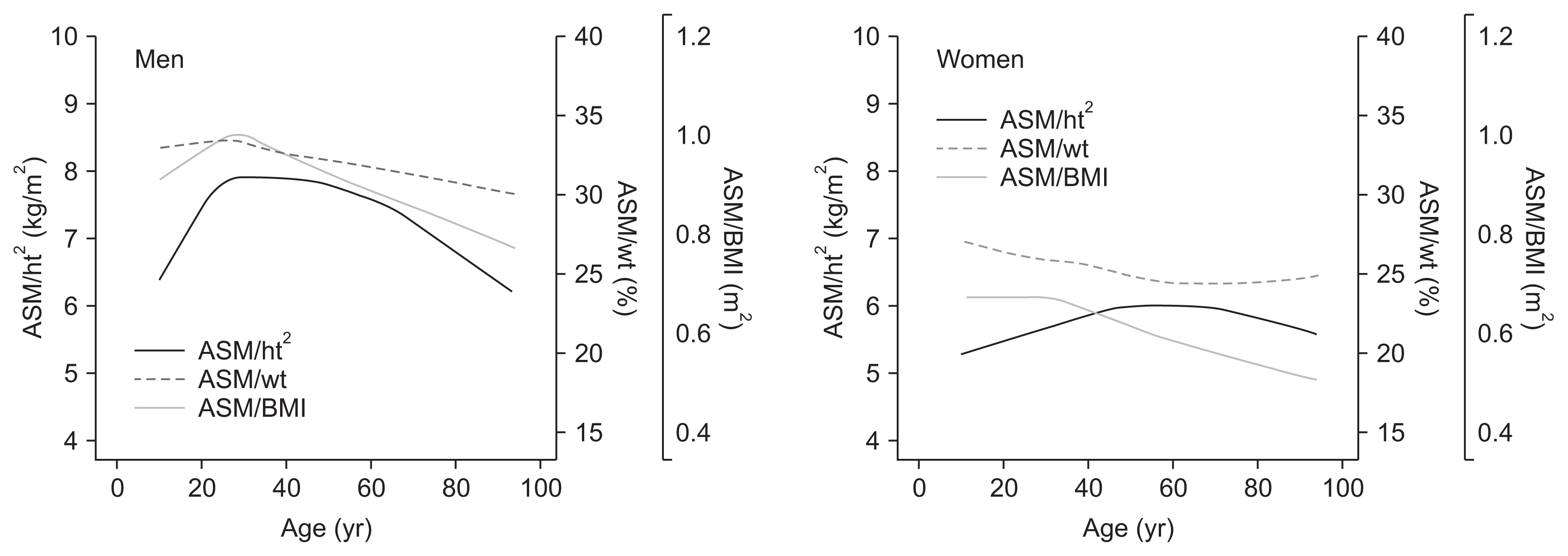
The total muscle mass and ASM in Korean men increases rapidly until their 30s and then decreases continuously until 90 years of age, with a slight acceleration after 60 years of age.33) This finding is similar to that for men in Western countries.9,10) However, total muscle mass and ASM in women increases slowly until their 40s, remains constant until their 50s to 60s, and then begins to decrease (Fig. 3). The age trends for the height-adjusted and BMI-adjusted ASM were similar to that of age-related change of ASM in Korean men (Fig. 4). However, in women, the age trend of muscle mass indices was substantially different among the height-adjusted, weight-adjusted and BMI-adjusted ASM. The peak of the height-adjusted ASM in women was around their 60s. This trend was different from that of Western countries. Thus, the low prevalence of sarcopenia by height-adjusted ASM in Korean older women is associated with a lower height-adjusted ASM of young reference in the Korean women.
Regarding the prevalence of sarcopenia using only skeletal muscle mass indices in Korean older people, the age trend in the prevalence of sarcopenia was commonly observed in all three indices in men (Fig. 2). However, the prevalence of sarcopenia was 2 fold higher for the BMI-adjusted ASM using the FNIH criteria compared to that of height-adjusted ASM in the same age groups. The increasing trend in the prevalence of sarcopenia with aging was observed using BMI-adjusted ASM in Korean older women. These findings suggest that BMI-adjusted ASM might be a more appropriate skeletal muscle mass index in Korean older adults, although further studies are needed to determine the cutoff points for sarcopenia in this population.
The Sarcopenia Study Group of Korean Geriatrics Society tried another approach for the diagnostic criteria of sarcopenia. They analyzed three cohort studies in Korea including the KNHANES, Korean Longitudinal Study of Health and Ageing and the Korean Genome and Epidemiology Study.32) These studies used DXA to measure the ASM. There was a slight difference in mean age, but the mean ASM and ASM/height2 were similar in each gender among the 3 studies (Table 2). They suggested the lowest quintile of height-adjusted ASM of the KNHANES as a cutoff point for the diagnosis of sarcopenia in Korean older adults because the KNHANES was a nationwide and population-based study. The Sarcopenia Study Group of KGS recommends an operational definition of sarcopenia in Korean older adults as shown in Table 3.
The cutoff point for grip strength in Korean older adults was based on the 2015 Report of National Physical Fitness Survey from the Korea Institute of Sport Science.34) Recently, Yoo et al.35) reported cutoff values of grip strength in Korean older men and women of 28.6 and 16.4 kg, respectively, using data from the KNHANES VI. Further studies are necessary to determine the cutoff points for Korean older adults. The cutoff point for gait speed in Korean older adults was adopted from the AWGS because there is currently no available representative study on gait speed in this population. Recently, Hong et al.36) demonstrated that the slower gait speed (<0.4 m/sec for 2.5 m) was associated with increased 3-year mortality using data from the Survey of Korean Elderly Status in 2008 and 2011. Jung et al.37) also showed that the first quartile of sex-specific gait speed (men, 0.663 m/sec; women, 0.545 m/sec) was associated with an increased risk of death or institutionalization in community-dwelling rural older people. These studies clearly demonstrated that the gait speed is an important predictor for poor health outcomes in Korean older people. However, further studies are needed to determine the optimal cutoff point of gait speed in this population.
SCREENING STRATEGY FOR SARCOPENIA IN KOREA
The EWGSOP recommends routine screening for sarcopenia among community-dwelling older people over 65 years of age by measuring gait speed.12) Meanwhile, the International Working Group on Sarcopenia (IWGS) suggests that sarcopenia should be evaluated in older patients with certain conditions including noted decline in function, strength, and health status; self-reported mobility-related difficulty; history of recurrent falls; recent unintentional weight loss (>5%); posthospitalization; and other chronic conditions.20) In addition, the IWGS recommends gait speed as a screening test and assessment of muscle mass by DXA in patients with a gait speed <1.0 m/sec.
The AWGS recommends screening for sarcopenia among community-dwelling older adults as well as older adults with certain clinical conditions in all healthcare settings,30) similar to IWGS recommendations. The AWGS also suggests grip strength and gait speed as screening tools, and that muscle mass in older adults with low grip strength and/or low gait speed should be assessed by DXA or BIA.
In Korea, there are no consensus or guidelines for the screening of sarcopenia in older adults. However, the recommendations of the AWGS are appropriate in this population. DXA is a better tool for the measurement of skeletal muscle mass because the assessment of skeletal muscle mass using BIA requires further research for application in Korean older adults.38)
CONCLUSION
With rapid population aging, there is a remarkable increase in the number of older adults in Korea. Sarcopenia, a progressive decline in muscle mass and strength, develops as a consequence of aging and may progress to frailty, loss of independence, physical disability, and increased mortality in older adults. Thus, sarcopenia has become a serious clinical problem in older adults. For the diagnosis and treatment of sarcopenia and the prevention of frailty or disability in older people, it is necessary to establish diagnostic criteria for sarcopenia in Korean older adults. In this review, I suggested a screening strategy and diagnostic criteria for sarcopenia for Korean older adults.